
- Center on Health Equity & Access
- Clinical
- Health Care Cost
- Health Care Delivery
- Insurance
- Policy
- Technology
- Value-Based Care
Profiles in Care: Importance of a Coordinated Health Care Plan in Plaque Psoriasis and Psoriatic Arthritis Management
With the shift to value-based reimbursement structures, coordinated care efforts (ie, the deliberate organization of patient care activities and information sharing across all care providers to achieve safer, more effective care) are being implemented across the health care spectrum to help optimize outcomes and reduce costs for patients, providers, and payers. The Institute of Medicine recognizes care coordination as a primary strategy to help enhance effectiveness, safety, and efficiency in the health care system.1,2 Patients with chronic, complex conditions, such as psoriasis and psoriatic arthritis (PsA), may experience particular benefit from the support offered through coordinated care frameworks. The following content and subsequent interviews describe the complexities associated with psoriatic disease and potential coordinated approaches that may help support outcomes for this patient population.
PSORIASIS OVERVIEW
Psoriasis is a relapsing inflammatory skin disease that affects more than 8 million adults in the United States.3-6 Approximately 90% of those with psoriasis have plaque psoriasis (PsO), which is characterized by clearly demarcated erythematous plaques with silvery scales that can present across the body surface.7 Typically, less than 3% body surface involvement is considered mild disease, 3% to 10% involvement is considered moderate, and greater than 10% involvement is severe.3
PsA affects women and men equally, with a prevalence of approximately 0.06% to 0.25% in the general US population.8 Of patients with psoriasis, approximately 20% to 30% develop PsA (as of 2019). The arthritic presentation of PsA can be extremely diverse; however, it commonly presents with peripheral arthritis and/or inflammation of ligaments and tendons (also known as enthesitis).4,8-11 PsA can lead to ongoing damage to the joints, diminished quality of life, and a higher mortality rate. It is also associated with higher rates of health care utilization and costs,9 contributing to the estimated $112 billion annual cost of psoriasis management in the United States.12
TREATMENT APPROACH FOR PSORIATIC CONDITIONS
Aggressive treatment results may be optimized by recognizing psoriatic diseases as a complex inflammatory disorder that affects many body systems—not only the skin—and that treatment can require a proactive, multifaceted approach.4,9 Although most patients with mild to moderate PsO can manage their condition with topical therapies or phototherapy, patients with moderate to severe PsO typically need systemic treatment.3,4 A combination of approaches is used in patients with PsA including nonpharmacologic therapies (eg, physical therapy, weight loss, and exercise) and pharmacologic therapies (eg, NSAIDs, oral disease-modifying anti-rheumatic agents, and biologics).9
It is important for patients with psoriatic disease to receive the right treatment at the right time. Early detection and early treatment may improve outcomes.9,13 Even a 6-month delay in PsA treatment can result in permanent joint damage and greater disability.14 Despite the importance of proactive treatment, psoriasis is often undiagnosed, undertreated, or not treated at all.4,15,16 According to results from a National Psoriasis Foundation survey, 52% of 4862 patients with psoriasis indicated dissatisfaction with their treatment.16 Treatment selection should involve consideration of therapies needed to manage the pain and comorbidities that often accompany psoriasis.
PAIN MANAGEMENT
Psoriatic disease is often accompanied by symptoms of skin or joint pain. Of patients with psoriasis, more than 40% experience skin pain and approximately 31% experience axial low back pain; however, pain is often underreported and therefore underrecognized.17 It can range from mild to severe, from superficial to deep, and may involve sensations such as tenderness, aching, cramping, or burning. Pain associated with PsA is particularly complex and is best managed through a multidisciplinary care team (including dermatologists, physical therapists, orthopedic surgeons, rheumatologists, and pain physicians) and a combination of therapies.17
COMORBIDITY CONSIDERATIONS
The complexity of psoriasis management may be attributed in part to its associated comorbidities, which include obesity, chronic kidney disease, Crohn’s disease, dyslipidemia, diabetes mellitus, metabolic syndrome, and psychiatric conditions.4,18 Cardiovascular comorbidities, such as hypertension, myocardial infarction, and stroke, necessitate regular screenings in patients with psoriasis and support early diagnosis and treatment. The complexity of managing psoriatic diseases, as well as the associated comorbidities, warrants streamlined communication among the dermatologist, primary care provider, and other specialists to ensure that patients receive optimal, comprehensive care with minimal fragmentation.18
Within dermatology, the psoriatic diseases are most strongly associated with psychiatric disorders, such as depression. The psychiatric comorbidities can be driven by behaviors and characteristics that often accompany psoriatic diseases (eg, physical disfigurement, social stigmatism, increased alcohol consumption, and dissatisfaction with treatment).19,20 In a meta-analysis that reviewed pooled data of more than 31,000 patients with PsA, results showed that depression was the most commonly studied mental health disorder (along with anxiety). Approximately 20% of the patients reported having at least mild depression, with the prevalence of overall depression ranging from 5% to 51% across different data sets. Those with depression reported greater disease activity.21 Notably, patients with PsA had a higher incidence rate of “any suicidality” than that of the general population, according to 1 of the studies reviewed.22 The authors noted a paucity of studies on this topic and that additional research is warranted.21
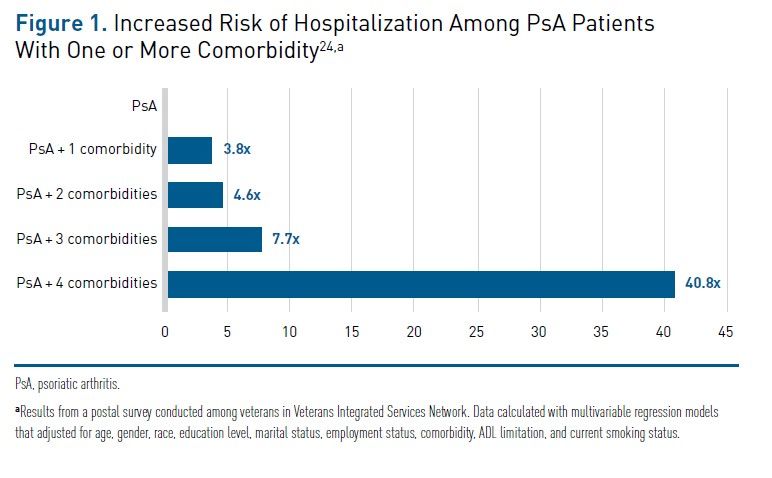
Patients with psoriasis who have comorbidities use more health care resources each year than do those without comorbidities. They are more likely to experience higher rates of urgent care visits, outpatient visits, and hospitalizations.23 For patients with PsA, the presence of 1 comorbidity can increase the probability of hospitalization by 3.8 times, and additional comorbidities increase the probability even more (Figure 1).24


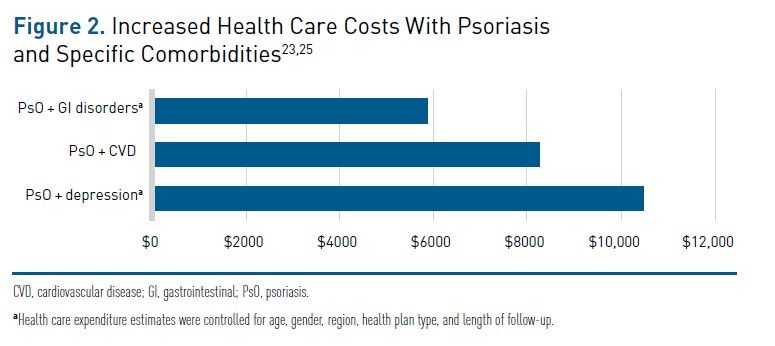
Comorbidities among patients with psoriasis also contribute to higher health care costs. In a retrospective cohort study on patients with psoriasis, results from a direct cost analysis (N=56,406) showed that the incremental adjusted annual direct cost experienced by patients with psoriasis with 1 comorbidity (of 10 comorbidities, including cardiovascular disease, depression, anxiety, diabetes, and obesity) was approximately $6639 more than that experienced by patients with psoriasis without a comorbidity, with cardiovascular disease associated with 1 of the greatest cost increases ($8275).23 According to results from another retrospective cohort study on patients with psoriasis (N=2489), depression was associated with an increased cost of $10,482 and GI disorders with an increased cost of $5867 (Figure 2).23,25


NEED FOR COORDINATED CARE AMONG PATIENTS WITH PSORIATIC CONDITIONS
With consideration to the complex, multisystem, inflammatory nature of psoriasis, its comorbidities (including high rates of psychiatric disorders), and its dependence on timely and appropriate treatment for optimal outcomes, patients with psoriasis may benefit from the multidisciplinary, patient-centered approach offered through coordinated care models.1 Components of a successful model can include comprehensive care and medication management across a multidisciplinary care team (eg, primary care physicians, nurses, dietitians, pharmacists, behavioral health specialists, rheumatologists, and dermatologists), shared patient information and disease tracking through health information technology (eg, electronic health records [EHRs]), and patient-centered education and self-management.1,2
QUALITY MEASURES TO INCENTIVIZE IMPROVED CARE OUTCOMES
As a part of the effort to improve psoriasis outcomes through a coordinated care model, providers can track quality measures via the qualified clinical data registry (QCDR) from the American Academy of Dermatology (AAD) to submit to the Centers for Medicare & Medicaid Services for Merit-based Incentive Payment System (MIPS) reporting. Individual AAD QCDR measures related to psoriasis for 2021 include the percentage of patients with psoriasis screened for PsA at each visit (AAD 7) and the percentage of patients with psoriasis aged 18 years or more, who, at the index visit, received a patient-reported itch severity assessment with a score of 4 or more and, at a follow-up visit, reduced the score by at least 2 points (AAD 9). Additional MIPS measures for patients with psoriasis include clinical response to systemic therapy (MIPs 410).26
CURRENT COORDINATED CARE EFFORTS IN DERMATOLOGY AND RHEUMATOLOGY
Several organizations have already begun to coordinate care between dermatology and rheumatology and have experienced positive results with their patients with PsO and PsA. Cleveland Clinic developed a collaborative dermatology-rheumatology clinic, which they noted has improved patient outcomes and enhanced research and education opportunities.27 Similarly, Brigham and Women’s Hospital developed the Brigham’s Center for Skin and Related Musculoskeletal Diseases, which offers patients with psoriatic disease comprehensive care from a single location. In the center, rheumatologists, with their expertise in joint examination and differential diagnoses for joint disorders, team with dermatologists, who navigate the various presentations of psoriasis and identify appropriate therapies for the skin.28 This collaborative approach is also supported in certain medical school academic programs, such as a dermatopathology residency program offered through the University of Virginia, which involves participation in a multidisciplinary rheumatology-dermatology clinic.29
Medical networks and groups have also been established to encourage collaboration among disciplines for the treatment of psoriatic disease. The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) supports “sharing of information related to psoriasis and PsA [and] networking among different medical disciplines that see psoriasis and psoriatic arthritis patients.”30 Even more specifically, the Psoriasis & Psoriatic Arthritis Clinics Multicenter Advancement Network (PPACMAN) aims to support partnerships between dermatologists and rheumatologists for psoriasis management, and has established a network of combined clinics that focuses on improving education regarding psoriatic disease, supporting additional formation of combined clinics, and researching the effectiveness of these models.31
ADDITIONAL OPPORTUNITIES FOR COORDINATED CARE
Although positive efforts are being made toward coordinating psoriasis care among dermatologists and rheumatologists, there are additional opportunities to coordinate care across the entire health care spectrum for patients with psoriatic disease. According to the Global Psoriasis Coalition, it may be beneficial to include primary care providers (PCPs) in the coordinated care model; with high-frequency patient contact, PCPs are well positioned to oversee and coordinate the facets of patient care outside of dermatology and rheumatology. Centralized providers—whether they be PCPs or combined dermatology-rheumatology clinics—can help ensure treatment adherence, screen for common comorbidities, connect patients to additional specialists and community resources, monitor for changes in disease severity, offer patient education, and assess the psychological impact of PsO or PsA on the patient. These centralized providers can also ensure open and ongoing communication with patients to clarify their preferences and track their satisfaction with treatment and outcomes; the providers can then liaise with involved specialists—such as cardiologists or behavioral health specialists—to ensure a patient-centric and coordinated approach across the entire patient care spectrum.32
EXPERT PERSPECTIVES IN COORDINATED HEALTH CARE
Fundamental aspects of coordinated care are applicable across many fields of chronic disease, and providers who want to develop a coordinated approach for psoriasis care may benefit by reviewing management strategies employed by other health care sectors. The following interviews branch into various sectors (primary care and psychiatry) to glean insights on how they approach care coordination and the patient and organizational priorities they have established for optimized care.
REFERENCES
- Care coordination. Agency for Healthcare Research and Quality website. Updated August 2018. Accessed May 17, 2021. https://www.ahrq.gov/ncepcr/care/coordination.html
- Gionfriddo MR, Pulk RA, Sahni DR, et al. ProvenCare-Psoriasis: A disease management model to optimize care. Dermatol Online J. 2018;24(3):13030/qt5xt2s05b.
- Menter A, Gelfand JM, Connor C, et al. Joint American Academy of Dermatology-National Psoriasis Foundation guidelines of care for the management of psoriasis with systemic nonbiologic therapies. J Am Acad Dermatol. 2020;82(6):1445-1486. doi:10.1016/j.jaad.2020.02.044
- Menter A, Strober BE, Kaplan DH, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol. 2019;80(4):1029-1072. doi:10.1016/j.jaad.2018.11.057
- Rachakonda TD, Schupp CW, Armstrong AW. Psoriasis prevalence among adults in the United States. J Am Acad Dermatol. 2014;70(3):512-516. doi:10.1016/j.jaad.2013.11.013
- Icen M, Crowson CS, McEvoy MT, Dann FJ, Gabriel SE, Maradit Kremers H. Trends in incidence of adult-onset psoriasis over three decades: a population-based study. J Am Acad Dermatol. 2009;60(3):394-401. doi:10.1016/j.jaad.2008.10.062
- Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386(9997):983-994. doi:10.1016/S0140-6736(14)61909-7
- Ogdie A, Weiss P. The Epidemiology of Psoriatic Arthritis. Rheum Dis Clin North Am. 2015;41(4):545-68. doi:10.1016/j.rdc.2015.07.001.
- Singh JA, Guyatt G, Ogdie A, et al. Special article: 2018 American College of Rheumatology/National Psoriasis Foundation guideline for the treatment of psoriatic arthritis. Arthritis Care Res (Hoboken). 2019;71(1):2-29.
- Mease PJ, Gladman DD, Papp KA, Khraishi MM, Thaçi D, Behrens F, Northington R, Fuiman J, Bananis E, Boggs R, Alvarez D. Prevalence of rheumatologist-diagnosed psoriatic arthritis in patients with psoriasis in European/North American dermatology clinics. J Am Acad Dermatol. 2013;69(5):729-735. doi:10.1016/j.jaad.2013.07.023
- Karmacharya P, Chakradhar R, Ogdie A. The epidemiology of psoriatic arthritis: A literature review. Best Pract Res Clin Rheumatol. 2021:101692. doi:10.1016/j.berh.2021.101692
- Brezinski EA, Dhillon JS, Armstrong AW. Economic burden of psoriasis in the United States:
a systematic review. JAMA Dermatol. 2015;151(6):651-658. doi:10.1001/jamadermatol.2014.3593 - Gladman DD. Early psoriatic arthritis. Rheum Dis Clin North Am. 2012;38(2):373-386. doi:10.1016/j.rdc.2012.05.005
- Haroon M, Gallagher P, FitzGerald O. Diagnostic delay of more than 6 months contributes to poor radiographic and functional outcome in psoriatic arthritis. Ann Rheum Dis. 2015;74(6):1045-1050. doi:10.1136/annrheumdis-2013-204858
- Kurd SK, Gelfand JM. The prevalence of previously diagnosed and undiagnosed psoriasis in US adults: results from NHANES 2003-2004. J Am Acad Dermatol. 2009;60(2):218-224. doi:10.1016/j.jaad.2008.09.022
- Armstrong AW, Robertson AD, Wu J, Schupp C, Lebwohl MG. Undertreatment, treatment trends, and treatment dissatisfaction among patients with psoriasis and psoriatic arthritis in the United States: findings from the National Psoriasis Foundation surveys, 2003-2011. JAMA Dermatol. 2013;149(10):1180-1185. doi:10.1001/jamadermatol.2013.5264
- Kodumudi V, Rajput K. Pain management in painful psoriasis and psoriatic arthropathy: challenging and intricately intertwined issues involving several systems. Curr Pain Headache Rep. 2021;25(6):36. doi:10.1007/s11916-021-00952-5
- Smith J, Cline A, Feldman SR. Advances in Psoriasis. South Med J. 2017;110(1):65-75. doi:10.14423/SMJ.0000000000000596
- Ferreira BI, Abreu JL, Reis JP, Figueiredo AM. Psoriasis and associated psychiatric disorders: A systematic review on etiopathogenesis and clinical correlation. J Clin Aesthet Dermatol. 2016;9(6):36-43.
- Rieder E, Tausk F. Psoriasis, a model of dermatologic psychosomatic disease: psychiatric implications and treatments. Int J Dermatol. 2012;51(1):12-26. doi:10.1111/j.1365-4632.2011.05071.x
- Zhao SS, Miller N, Harrison N, et al. Systematic review of mental health comorbidities in psoriatic arthritis. Clin Rheumatol. 2020;39,217–225. https://doi.org/10.1007/s10067-019-04734-8
- Wu JJ, Penfold RB, Primatesta P, et al. The risk of depression, suicidal ideation and suicide attempt in patients with psoriasis, psoriatic arthritis or ankylosing spondylitis. J Eur Acad Dermatol Venereol. 2017;31(7):1168-1175. doi:10.1111/jdv.14175
- Feldman SR, Tian H, Gilloteau I, Mollon P, Shu M. Economic burden of comorbidities in psoriasis patients in the United States: results from a retrospective U.S. database. BMC Health Serv Res. 2017;17(1):337. doi:10.1186/s12913-017-2278-0
- Singh JA, Strand V. Health care utilization in patients with spondyloarthropathies. Rheumatology (Oxford). 2009;48(3):272-276. doi:10.1093/rheumatology/ken472
- Crown WH, Bresnahan BW, Orsini LS, Kennedy S, Leonardi C. The burden of illness associated with psoriasis: cost of treatment with systemic therapy and phototherapy in the US. Curr Med Res Opin. 2004;20(12):1929-36. doi:10.1185/030079904X15192
- 2021 quality measures for MIPS reporting. American Academy of Dermatology Association website. Accessed June 2, 2021. https://www.aad.org/member/practice/mips/measures/2021
- Collaborative rheumatology-dermatology clinic improves outcomes. Cleveland Clinic website. Published November 6, 2020. Accessed June 6, 2021. https://consultqd.clevelandclinic.org/collaborative-rheumatology-dermatology-clinic-improves-outcomes
- Rheumatology-dermatology collaboration enhancing PsA care. Brigham and Women’s Hospital website. Accessed June 6, 2021. https://www.brighamhealthonamission.org/2021/01/27/rheumatology-dermatology-collaboration-enhancing-psa-care/
- Clinical training. University of Virginia School of Medicine website. Accessed June 6, 2021. https://med.virginia.edu/dermatology/residency-program/clinical-training/
- What’s new at GRAPPA. GRAPPA website. Accessed June 6, 2021. Grappanetwork.org
- About us. PPACMAN website. Accessed June 6, 2021. www.ppacman.org/about.html
- Psoriasis & primary care report. Global Psoriasis Coalition. Published September 2019. Accessed June 2, 2021.https://static1.squarespace.com/static/5bc59291a5682766916e321b/t/5d88ed985927590d6ab7470e/1569254808740/Psoriasis+and+Primary+Care+Report_FINAL.pdf


