
- Center on Health Equity & Access
- Clinical
- Health Care Cost
- Health Care Delivery
- Insurance
- Policy
- Technology
- Value-Based Care
Pharmacoeconomics Refresher: The CVS $100K/QALY Announcement (Part 1)
This series of pharmacoeconomics posts will explore the meaning of $100,000/quality-adjusted life year (QALY) and why it might matter to these 4 P’s: patients, payers, providers, and pharma. Part 1 focuses on definitions and a basic calculation.
In a recent announcement, CVS Health shared their new approach to making drugs more affordable which included 3 new strategies:
- Zero Out-of-Pocket Costs for Chronic Disease
- Reducing Launch Price Using Comparative Effectiveness
- Transparency in Drug Costs
One of the messages in the “reducing launch price” section that has caught some negative attention from a few stakeholders focuses on this paragraph:



This series of pharmacoeconomics posts will dissect this paragraph with the aim of educating a broad The American Journal of Managed Care® audience on the meaning of $100,000/quality-adjusted life year (QALY) and why it might matter to these 4 P’s: patients, payers, providers, and pharma. Part 1 focuses on definitions and a basic calculation, part 2 puts the economics calculation into a decision-making context, and part 3 discusses why it matters.
ICER and ICER
When discussing “cost-effectiveness” in the context of healthcare, researchers focus on study designs such as cost-of-illness, cost-effectiveness analysis (CEA), cost-utility analysis (CUA), and cost-benefit analysis—for more in-depth reading on each type of analysis, I’d recommend getting a copy of the Drummond et al. text book. The recommended results reported in a CEA or CUA study is called an incremental cost-effectiveness ratio (ICER). This is because we are comparing a new treatment against an older treatment (or no treatment) so that we can focus on this incremental impact. The Institute for Clinical and Economic Review (also commonly called “ICER”) was founded in 2006 as an independent research organization to conduct these CEA/CUA type studies. They also refer to themselves as “the nation’s independent watchdog on drug pricing.” Thanks to this clever marketing, anyone having a serious discussion about economic analyses and the resulting ICER of a drug may also confuse people with the acronym of one of the largest groups calculating them.
As for the ratio itself, an ICER can be described like this:


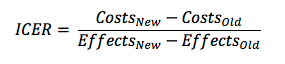
From a conceptual standpoint, the ICER is really simple and straightforward. The real fun begins when a researcher begins to determine which “costs” and which “effects” to count for this equation.
Health Effectiveness as QALYs
If researchers conducting cost-effectiveness studies formed a nation, the Panel on Cost-Effectiveness in Health and Medicine would be analogous to the Supreme Court—they are a highly respected group of individuals who were originally gathered in 1993 by the US Public Health Service to establish guidelines on these types of studies. A Second Panel was convened to update the original panel’s recommendations and published their results in 2016. In both cases, the cost-effectiveness Supreme Court ruled that an ICER should “measure health effectiveness in terms of QALYs” for a variety of reasons.
What is a QALY?
Sarah Whitehead and Shehzad Ali did a fantastic job explaining the QALY and how it is typically derived in 2010, so for the extra-curious reader I’d recommend reading it. The QALY enables the researcher to incorporate morbidity into the measure. Without considering quality of life, any treatment that doesn’t extend life could be considered worthless.
Fun QALY Math
For us to mathematically compare 2 health situations based on expected quality of life, like perfectly healthy vs sick, we could set perfectly healthy=1 and sick=0.5 (referred to as a utility measure in the analysis). So, when we compare 2 people receiving different treatments with 1 person who remains perfectly healthy for 10 years after Treatment A and another person who is sick for 10 years after receiving Treatment B, we multiply our quality of life adjustments to get: 10 years x 1 = 10 QALYs vs. 10 years x 0.5 = 5 QALYs. Even though both people lived 10 additional years, we would say that the first person who received Treatment A gained 5 additional QALYs.
Putting QALY in an ICER
Now when we bring our health effects (calculated as QALYs) back to determine the cost-effectiveness of Treatment A vs. Treatment B, we start setting up our equation with all of our costs and effects. For this example, let’s assume that Treatment A costs $10,000 and all other costs included during the 10-year observation period, including things like follow-up doctor visits and productivity costs, added another $10,000, totaling $20,000 of costs for Treatment A. The cost of Treatment B was only $2000, but the costs during the next 10 year period when the person was sick was $13,000, bringing our total costs for Treatment B to $15,000. When we plug in our costs and effects into our ICER it would look like this:



So we have calculated an ICER…now what? Be sure to check out Part 2 as we start to translate our ICER into a decision-making context.

















