- Center on Health Equity & Access
- Clinical
- Health Care Cost
- Health Care Delivery
- Insurance
- Policy
- Technology
- Value-Based Care
Insurance Gaps Threaten Cancer Treatment Success
Access to and affordability of immune checkpoint inhibitors, which can be lifesaving if patients receive them on time and under optimal circumstances, continue to top the list of reasons behind outcomes disparities for patients who have private insurance vs those who remain uninsured.
Although intended to improve outcomes for patients living with 1 of 3 stage IV cancer types—melanoma, non–small cell lung cancer (NSCLC), or renal cell carcinoma (RCC)—immune checkpoint inhibitors (ICIs) may not confer equivalent survival benefits among individuals who have 1 of 2 insurance types—private insurance or Medicaid—or are uninsured. New cross-sectional study results paint a picture of widening survival disparities, favoring patients who have private insurance over those who are not insured.
ICIs act as brakes for the T cells of the immune system, preventing them from speedily destroying healthy cells as they work to attack cancerous T cells. When ICIs are effective, they block immune checkpoint proteins on healthy T cells from binding with their so-called partner proteins on tumor cells, thereby enabling the destruction of cancer cells.1
Findings were published online July 7 in JAMA Network Open from an analysis of patients identified using National Cancer Database data with new diagnoses of stage IV melanoma (n = 12,048), NSCLC (n = 152,610), or RCC (n = 18,782) before and after the FDA approved ICIs; mortality data were provided by the Surveillance, Epidemiology, and End Results program.2 The authors’ time period was January 1, 2002, through December 31, 2019. On March 25, 2011, ipilimumab was the first ICI to be approved, with indications encompassing unresectable or metastatic melanoma.3
The primary outcome was 2-year overall survival. Less than half of the patients were women (43.5%), the mean (SD) overall age was 55.5 (7.0) years, and most patients were aged 50 to 59 or 60 to 64 years (83.5%), lived in an area with a population of at least 1 million (48.5%) or less than 1 million (31.0%), were considered middle class (84.3%), reported a non-Hispanic White race and ethnicity (77.0%), and were treated through a community cancer program (34.1%) or a teaching/research hospital (23.0%).
Of the entire study population (n = 183,440), 65% had private insurance, 24% had Medicaid, and the rest had no coverage at diagnosis; however, more than 81% of patients with each cancer type still received treatment. NSCLC was the most common cancer seen (83.2%), and melanoma (6.6%) was the least. With private health insurance as the reference, survival percentages were up across the board for the 3 cancer types and the 3 insurance categories, comparing the pre-ICI and ICI eras (TABLE2).


Table
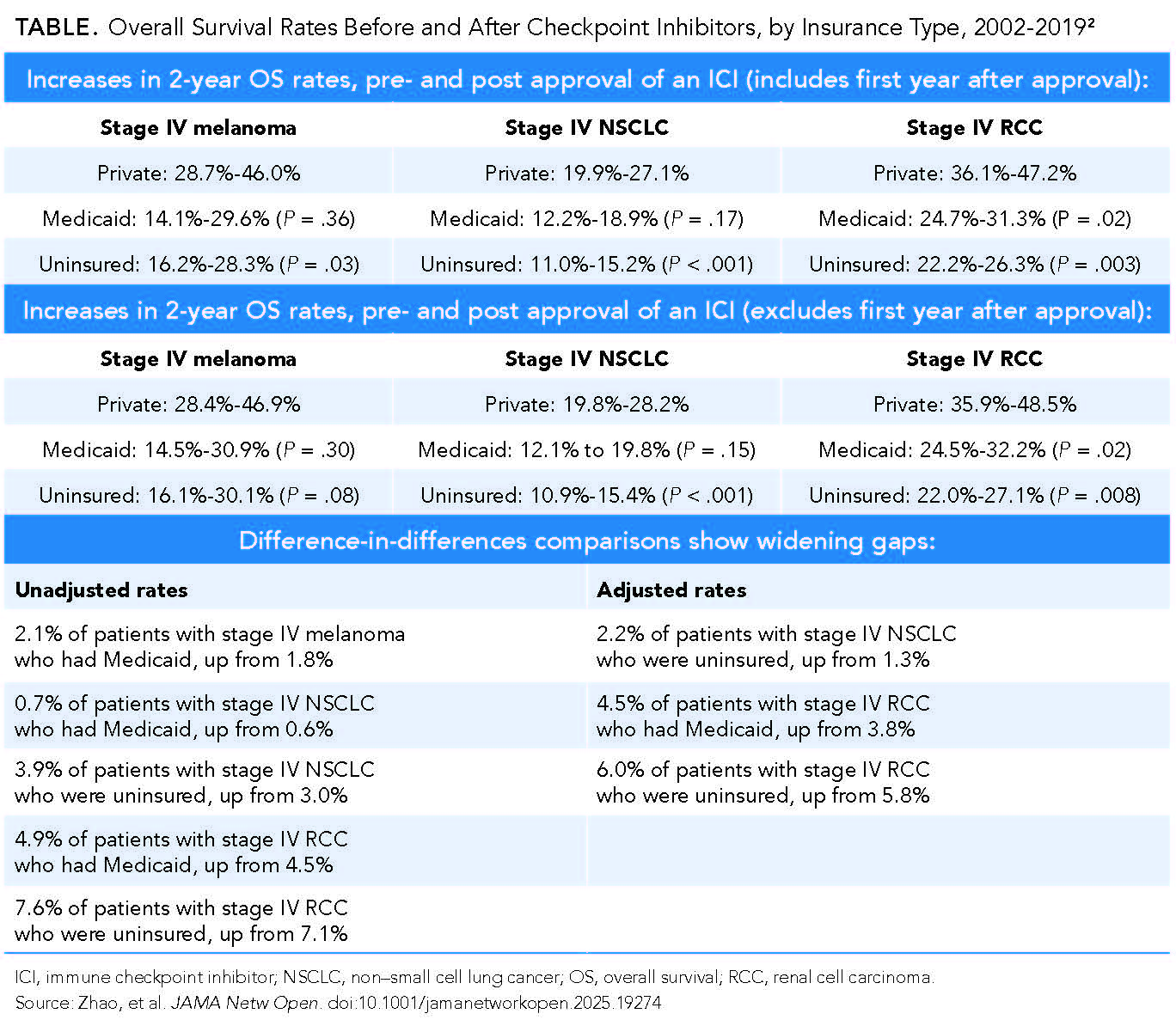
However, as shown, the difference-in-differences data paint a different picture. Looking at the unadjusted and adjusted totals of percentages of patients who survived, the survival gaps widened for several patient populations.
“Our findings have significant implications in the context of long-standing disparities in cancer outcomes in the US, where individuals with lower socioeconomic status or without health insurance have experienced worse survival rates,” the authors wrote, with the policy implications being significant. They explained that these outcome disparities might only serve to worsen as the cancer treatment landscape of ICIs continues to change, but that hope lies in the similar survival rates of those with private insurance and those who benefited from expanded Medicaid coverage under the Affordable Care Act, “suggesting that expanding Medicaid to individuals without health insurance
coverage may improve their access to ICI treatment.”
Additional avenues to expanded access are financial assistance and patient navigation programs, particularly in cases where out-of-pocket costs remain high. It would be nice, too, for these treatments to be more affordable. Also, future research should examine the impact of insurance coverage changes on treatment access.
There are several limitations on these findings. Health insurance status was only evaluated at diagnosis; coverage changes were not accounted for. Also, cancer-specific mortality was not considered, only all-cause mortality; only 3 cancer types were included; and data were not available on specific treatment agents, limiting the authors’ analysis to a population level only.
References
1. Immune checkpoint inhibitors. National Cancer Institute. Updated April 7, 2022. Accessed July 5, 2025. https://www.cancer.gov/about-cancer/treatment/types/immunotherapy/checkpoint-inhibitors
2. Zhao J, Graetz I, Howard D, Yabroff KR, Lipscomb J. Immune checkpoint inhibitors and survival disparities by health insurance coverage among patients with metastatic cancer. JAMA Netw Open. 2025;8(7):e2519274. doi:10.1001/jamanetworkopen.2025.19274
3. FDA approves Yervoy (ipilimumab) for the treatment of patients with newly diagnosed or previously-treated unresectable or metastatic melanoma, the deadliest form of skin cancer. News release. Bristol Myers Squibb. March 25, 2011. Accessed July 5, 2025. https://news.bms.com/news/details/2011/FDA-Approves-YERVOY-ipilimumab-for-the-Treatment-of-Patients-with-Newly-Diagnosed-or-Previously-Treated-Unresectable-or-Metastatic-Melanoma-the-Deadliest-Form-of-Skin-Cancer/default.aspx