
- Center on Health Equity & Access
- Clinical
- Health Care Cost
- Health Care Delivery
- Insurance
- Policy
- Technology
- Value-Based Care
Digital Health Solutions in Chronic Illnesses: An AJMC® Scientific Interchange
In September 2022, a diverse group of health care decision makers convened for a Scientific Interchange hosted by The American Journal of Managed Care®. The event was moderated by Jessica Hauflaire, chief operating officer at Digital Therapeutics Alliance in Seattle, Washington. Five faculty participated: Louis Christos, RPh, pharmacy director at a regional health plan based in Connecticut; Nihar R. Desai, MD, MPH, vice chief of the section of cardiovascular medicine, investigator at the Center for Outcomes Research and Evaluation, and associate professor at Yale School of Medicine in New Haven, Connecticut; Steven Evans, MD, chief medical officer at Centene in Las Vegas, Nevada; Eugean Jiwanmall, MPH, MBA, senior research analyst for medical policy and technology evaluation at Independence Blue Cross in Philadelphia, Pennsylvania; and Eric Cannon, PharmD, chief pharmacy officer at SelectHealth and general manager at Scripius in Murray, Utah. During their discussion, the group explored key differences among digital health technology, digital medicine, and prescription digital therapeutics; a potential framework for evaluation of digital therapeutics; payer decision-making in creation of coverage policies for digital therapeutics; and emerging health care policies around reimbursement of digital health technology.
Definitions, Core Principles, and Classification of Digital Therapeutics
Digital therapeutics differ from digital health and digital medicine in that they deliver evidence-based therapeutic interventions to prevent, manage, or treat disease.1,2 Digital health includes technologies, platforms, or systems that enable data capture, storage, and transmittal of lifestyle, wellness, or health-related information about participants. Digital health products are not required to demonstrate clinical evidence supporting their use. Examples include health information technology (eg, electronic health records), telehealth visits, and clinical decision support software. Digital medicine refers to software or hardware products that measure or intervene with patients’ health; such products are required to provide clinical evidence for their use. Examples include digital diagnostics, remote patient monitoring, and digital products that measure and intervene (but do not need intervention to function).
Digital therapeutics are driven by software programs and data and may be used independently or in combination with other medications, devices, or therapies. Digital therapeutics are subject to review and clearance by regulatory bodies to support product claims, and they incorporate patient privacy and security protections. Some of the current key therapeutic areas for digital therapeutics include mental health, respiratory diseases, metabolic conditions, and chronic pain.2
The Digital Therapeutics Alliance has established the following foundational principles, all of which must be met for any product claiming to be a digital therapeutic3:
- prevent, manage, or treat a medical disorder or disease;
- provide medical intervention driven via software;
- incorporate best practices in design, manufacture, and quality;
- engage end users in development and usability processes;
- incorporate patient privacy and security protections;
- apply product deployment, management, and maintenance best practices;
- publish trial results inclusive of clinically meaningful outcomes;
- be reviewed and cleared and/or approved by regulatory, as required for claims;
- make claims appropriate to clinical validation and regulatory status; and
- collect, analyze, and apply real-world evidence and/or product performance data.
Digital therapeutics that meet industry core principles are classified into 1 of 3 categories based on the product’s primary purpose: (1) prescription therapeutics that treat a disease; (2) prescription or nonprescription therapeutics that manage a disease; or (3) prescription or nonprescription therapeutics that improve a health function. Digital medicine products also may be used in the diagnosis and evaluation of a disease.2 A digital therapeutic must deliver a therapeutic intervention and use clinical end points (eg, results from clinical trials and ongoing evidence generation) to support product claims.4
When evaluating digital therapeutics, payers and providers need to consider an array of access and utilization factors. In terms of access, payers must consider patients’ product access via a third-party payer, screening to determine appropriate access, need for provider authorization (eg, prescription referral), product delivery to the patient, access to a platform for product use, and the need for ancillary components for use (eg, wearable technology, sensors, or hardware). In their evaluation of a digital therapeutic, payers must assess product ease of use and scalability, appropriateness of care, patient engagement and retention, and privacy and security needs. Additionally, the digital therapeutic should provide value to all of those involved (eg, patients, caregivers, and providers) by demonstrating positive health outcomes, lowering overall costs, and supplying the patient and population with health benefits. Providers must ensure appropriate product utilization in terms of the indication, individual patient, specific therapy, timing and frequency of product use, documentation of outcomes, response to therapy, and evaluation of insights and data to assess and optimize therapy overall.3
Digital therapeutics are becoming an essential component of health care delivery systems because they can address critical gaps in care for underserved populations regardless of patient age, language, culture, income, disease state, or geography. Digital therapeutics can close health care gaps by providing therapies via smartphones, tablets, and other technologies; improving accessibility to therapies with demonstrated efficacy and safety; reducing the stigma associated with various therapies by supplying at-home delivery and privacy; and expanding providers’ reach to manage patients. In addition, digital therapeutics can close communication gaps by providing therapies in a variety of languages and generating valuable information and insight on individual goals and results to patients and their providers.5
Roundtable participants reported a range of experience with digital therapeutic products, from minimal to in-depth. Participants also recognized the distinction between digital therapeutics and digital health. Christos noted that continuous blood glucose monitors may be considered the original digital therapeutic. He also mentioned a software program for patients with opioid use disorder, as well as the pipeline of products in attention deficit-hyperactivity disorder (ADHD), irritable bowel syndrome, and migraine. The participants agreed that payers are keeping an eye on digital therapeutics; however, Christos explained that “[digital therapeutics] make up a small portion of what we are responsible for every day.” Evans reported involvement in a larger study of an app that monitored blood pressure and included a health coach component, as well as a physical therapy digital therapeutic that was “used quite a bit through Humana for our patients.” According to Jiwanmall, even before the COVID-19 pandemic, interest in digital therapeutics among payers had increased. “[We are] reviewing evidence and developing policy. It is a big deal at the current time.” Cannon agreed that digital therapeutics are a “big deal” clinically and for the health care system, but he noted that there is no existing framework for assessing a digital therapeutic’s effectiveness, coverage, reimbursement, clinical utility, and economic value for payers, providers, and health systems. “Just because something is new does not mean that it is better,” Cannon said. “There is a standard for assessing a new drug, device, [or] digital therapeutic. For clinicians, that standard of evidence is very important. That is the way we have been trained regarding decision-making and patient care.” Other participants agreed that such a framework is missing and that it is, indeed, a crucial part of evaluating a product so that pertinent questions can be answered; without it, the digital therapeutic could be overlooked or dismissed by decision-makers due to uncertainties related to clinical utility and cost.
According to the participants, the challenges with digital therapeutics include the sheer influx of available apps, reimbursement requests for subjective patient-reported data (that few providers or payers will have time to review and act on), and liability if a provider does not act on data that qualify as an emergency, such as a hypoglycemic event. Evans explained that “for me and for others, the bar is quite a bit higher in terms of acceptance of a digital therapeutic because we are not used to it.” Evans shared with the group what he learned from his experience with the aforementioned physical therapy digital therapeutic—that it does, in fact, work for some patients, but one has to identify the right type of patient who will benefit. Skepticism exists about the novelty, value, and even FDA approval of digital therapeutics. Indeed, FDA approval of a digital therapeutic carries less weight with some payers than it would for a drug product, which is perceived to be reviewed with more rigorous standards. Jiwanmall underscored that the digital therapeutic class is not going away, and uptake will continue to increase, particularly in a post–COVID-19 era in which virtual visits and telemedicine have become standard. As such, decision makers need to narrow their focus to a product’s clinical intent and utility in a well-defined subpopulation of patients.
Value of and Access to Digital Therapeutics
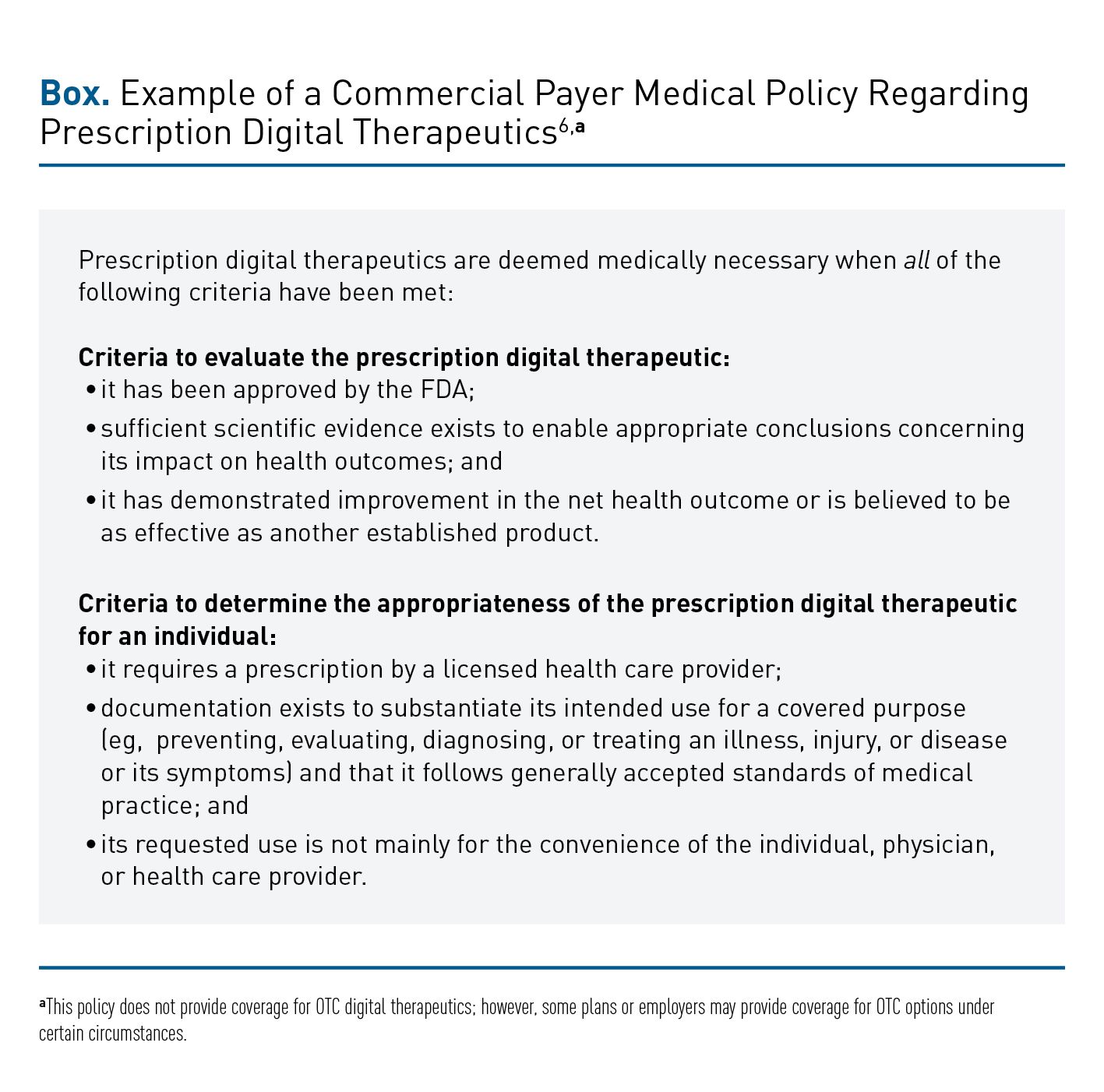
Participants discussed the value of digital therapeutics and their experiences in evaluating prescription and nonprescription digital therapeutics. The participants noted that, in their experience, commercial payers are inclined to not cover digital therapeutics that do not require a prescription or physician oversight, whereas Medicaid plans look to include some nonprescription digital therapeutics as value-added benefits. According to Christos, the value of a digital therapeutic is based on clinical evidence, and it should be supported by outcomes data. Currently, his plan does not have an overarching policy regarding digital therapeutics; however, each one is reviewed independently, and the manufacturer bears the burden of demonstrating the value of its intervention to plan decision makers. Christos discussed a video game that is a prescription treatment option for patients with ADHD; the results of a study showed that its efficacy was comparable with that of stimulant therapy. According to Christos, the efficacy results demonstrate the value of the digital therapeutic in terms of replacing a stimulant for a patient who does not want to use a controlled substance. If the digital therapeutic does not “improve any outcomes, I’m not sure there is any value,” said Christos. Evans added that value is a new concept for digital therapeutics. The classical definition of therapeutic value—that is, “the benefit minus the risk divided by the cost”—might need to be adjusted because digital therapeutics have the potential to demonstrate additional value by “providing care where otherwise it would not be provided,” Evans remarked. Desai listed a host of features to consider in the value story for digital therapeutics, such as access, scalability, efficiency, and individualization, as well as their potential to exacerbate existing health care disparities. “Not everyone has access to Wi-Fi or a smartwatch, [and these] things are not equally distributed in society,” he cautioned. “We should be very clear about the potential downsides of some of these [therapeutics].” Jiwanmall acknowledged that ensuring health equity in digital therapeutic access is an important goal; however, before that is achieved, payers need frameworks and evidence to evaluate the efficacy, safety, and quality of these products to meet clinical goals. Some payers have, or are developing, medical policies related to coverage of prescription digital therapeutics. An example of a commercial payer policy is shown in the Box.6


Although plan or employer coverage of a digital therapeutic may minimize access issues for some, providers still have the potential to be the rate-limiting step in their use. Because digital therapeutics represent a new model of care delivery, additional personnel and training may be necessary in some instances or with certain digital therapeutics. Cannon pointed out that, with digital therapeutics, “we suddenly provide a new and different burden on providers that may be outside of the realm of [their current training].” Evans noted that digital technology is not for everyone. Although a digital therapeutic may be beneficial for a certain segment of a population, individual factors to be considered may include the patient’s literacy level, manual dexterity, and cognitive ability. Moreover, access to digital therapeutics may be limited based on these individual factors, so there may be concern among payers that product access would not be equitable across a plan population. More broadly, a single digital therapeutic intervention will not work for everyone in a population and there is some individualization needed, just as a single drug may not be effective in the entire population, and a patient may have to try a few different therapies before finding the one that is right for them.
Among patients with Medicaid, digital therapeutic access via smartphones and Wi-Fi may be less of an obstacle than perceived, as some Medicaid plans provide free phones to plan members. Cannon remarked that it is easier to solve digital disparities than other types of disparities, such as lack of access to transportation for an office visit to a medical provider.
Conversely, Jiwanmall explained that the commercial vantage point is vastly different, and “there [likely] won’t be an appetite to adopt [digital therapeutics]” on a grand scale. He predicted that in the commercial realm, digital therapeutics will be evaluated closely in terms of routine care and the target patient population. Those digital therapeutics that demonstrate an improvement in outcomes over the existing clinical equivalent may be added to the policy; however, it will not total hundreds or even dozens of products at a given time.
A few participants mentioned that some plans’ executives may exert pressure to adopt digital therapeutics to demonstrate value-added benefits for Medicaid populations. Also, manufacturers could exert pressure in the form of advertising to patients. Desai shared that providers may be placed in an awkward position when patients inquire about a digital therapeutic, particularly when those individuals are doing well without one.
Assessing and Integrating Digital Therapeutic Products
The future of digital therapeutics will depend on the ability of companies to overcome fundamental challenges, including, as a study conducted by Deloitte revealed, whether they can show benefit through clinical and real-world evidence, achieve optimal pricing and reimbursement outcomes, and evaluate patients’ and providers’ experiences.2
Demonstration of Benefit
Digital therapeutics manufacturers must be able to demonstrate their products’ measurable benefits through clinical trials and real-world evidence. Providers may be unlikely to use these interventions if claims are not supported by sufficient published evidence.2 Efficacy, safety, and outcomes data (including costs) are necessary to convince decision makers to adopt digital therapeutics.
Optimization of Pricing and Reimbursement Outcomes
The roads to market access for digital therapeutics are poorly defined in some global regions, and reimbursement and coverage complexities (eg, confusing or insufficient requirements) are difficult to navigate in most areas. Still, digital therapeutics can give manufacturers and payers a chance to try innovative payment models (eg, pay-for-performance or outcomes-based contracts), given the plethora of real-world data.2
Evaluation of the Experience
Skepticism remains about the use of digital therapeutics products. Some of this skepticism is based on the perceptions that patients may try out the technology but lose interest over time and that those in higher socioeconomic classes may be more likely than those in lower socioeconomic classes to purchase and use these technologies. Furthermore, there are concerns about the use of personal health data, particularly as related to real-time monitoring features. There is also skepticism related to issues such as the need to modify processes regarding data acquisition and assessment, which might require additional staff training and place extra burden on the health care system.2
Integration of Digital Therapeutics
Digital therapeutics offer the potential to personalize treatment, extend or augment therapeutic offerings, improve health outcomes, and provide real-time clinical information and real-world data to inform care. Several key questions remain regarding integration of digital therapeutics, including whether the therapeutic requires a prescription, what types of capabilities the end user needs for appropriate use, how ongoing evidence will be generated, and whether the therapeutic complements existing therapy.2 With regard to evaluating products, Cannon and Desai shared their concerns about digital therapeutics being approved by the FDA despite many of these products lacking clinical study evidence in subpopulations (or a comparable standard) to demonstrate efficacy and safety that is required by the agency for drug and device approval. Jiwanmall said that “[full] acceptance and adoptability [of digital therapeutics] will come only when the uncertainties become certainties, and [that] can only [happen] if we are truly trying to do evidence-based medicine.”
In terms of cost from the commercial plan vantage point, Jiwanmall commented, “economic evaluation comes into play only after medical necessity has been set.” In other words, payers will look to evaluate the cost of a digital therapeutic only if it is as efficacious and safe as other therapeutic options available, including drugs and/or other more traditional treatment options; has evidence to support medical necessity; and can be integrated into routine clinical care. Jiwanmall emphasized, “First, we establish medical necessity, and then [we consider] the cost component.” Cannon countered that Jiwanmall’s health plan is in the minority and that most other health plans do not conduct product evaluation in this manner. Christos noted that cost is one of the biggest factors that arise when plans evaluate expensive products, such as gene therapies.
Evans has been the chairperson of pharmacy-and-therapeutics committees for 20 years, and he shared his experiences regarding product evaluation, saying, “You assume that something is medically necessary because it is FDA-approved and it has the studies.” A new product, he continued, is evaluated in the context of existing therapies and their cost-effectiveness: “You do not just say that this works really well [and] we will worry about the cost later.”
Jiwanmall clarified his earlier statement; cost, he said, becomes a consideration when the digital therapeutic and the existing nondigital therapeutic are clinically equivalent and covered by the plan, but there is a cost difference between the 2 products. Cannon and Desai agreed with Jiwanmall’s clarification, and Desai added that another “big piece to think about is health systems that are either self-insured or offering their own insurance products, [have] risk-bearing contracts, [or are part of an] accountable care organization [ACO]. Then we are managing risk, and we have to make our own independent adjudication [if] we want to provide something to our patients regardless of what commercial payers are doing.” He noted that the health system pathway may deviate from the traditional commercial plan pathway in terms of evaluating digital therapeutics. Jiwanmall agreed that plan funding—self-funded vs fully insured—will be a factor, as the former “may choose to not have the benefit” based on cost, medical necessity, and clinical evidence. He acknowledged that self-funded groups also may want to offer digital therapeutics outside of the plan’s policy. “All we can [do here is] provide them with a policy [and]... say, ‘This is the framework,’” Jiwanmall said.
Evans asked the group if they would consider evaluating and adopting a hypothetical digital therapeutic that had robust real-world evidence in diabetes and reduced the cost of care to their plan or health system by $15,000 to $20,000 per patient each year. Both Desai and Jiwanmall ardently agreed, with Desai admitting that he would “put it in my ACO tomorrow.” Evans rationalized that the participants would support this therapeutic because “it did something that improved care significantly enough that it improved the cost structure.” Both Evans and Jiwanmall respectfully disagreed and debated the extent to which data from randomized clinical trials vs real-world evidence factor into payers’ decisions to cover a product. Evans said, “When I look at the Blue Cross [policy information], I look at it for the clinical [data], but then I move on to what is really important”—that is, real-world evidence. He added, “if [a product] is FDA-approved, it [has] good studies, and in the real world it saves money, we adopt it.” Cannon proposed that imagination and creativity be used in the assessment and integration of digital therapeutics into health plans and health systems. “Every great advance that has happened in science and culture started with somebody stepping outside the rigidity of the existing system and building a model that is different,” he posited. Cannon also acknowledged that colossal failures have been a side effect of some of these great advances. Ultimately, the participants—and, more broadly, all payers, manufacturers, providers, and patients—are at a crossroads with digital therapeutics, which are developed, adopted, used, and propagated differently than are traditional therapies. Cannon suggested that the payers “take a step back and look at our evaluation models [rather than] keep ourselves in our rigid little box [and bypass] the chance to actually look at the massive opportunity that is out there.”
Regarding the main stakeholders involved in decision-making and procurement of digital therapeutics, Cannon shared that he has had conversations with digital therapeutic product owners, particularly those with profit and loss accountability, who conduct market value assessments to determine the value of early adoption vs late adoption of the therapeutic. Once these discussions and determinations are made, compliance, legal, and government regulatory discussions transpire. Determining whether a product falls under the pharmacy or medical benefit is another hurdle that must be overcome by decision makers. “I’ve taken the position [that] compliance figure[s] out what benefit it [falls under]. If it is filled at a pharmacy, I’m going to process [the product] under the pharmacy benefit, and, if I need to move dollars on the back end to bucket it under the right benefit, then we can do that,” said Cannon, adding that the benefit determination should not be the main barrier.
Medical vs Pharmacy Benefit of Coverage
Participants debated the pros and cons of covering a digital therapeutic under the pharmacy vs the medical benefit. Christos said that some manufacturers would likely want coverage under the pharmacy benefit because of real-time adjudication, patient access, and co-pay factors. Patient cost, the plan deductible, and product tier status must be factored into coverage decisions. For example, if a patient obtains a digital therapeutic at the start of the year when the plan deducible has not been met, a payer may not cover the product and the cost will be applied to the patient’s deductible. Yet, the patient will still be responsible for the full cost. Evans noted that the benefit type might not matter as much, stating, “[If] I need to move dollars [from the pharmacy side] to the medical side, I’ll do it, [and] it does not really matter. It is whatever makes sense in a particular situation.” Evans added that “our current policy is that [a digital therapeutic is covered] as a medical device would, so it’s [under the] medical [benefit].” Christos responded that stakeholders might want to advocate for how digital therapeutics will be covered, because, otherwise, every payer will cover these products differently. At present, Jiwanmall’s plan places digital therapeutics under the medical benefit; however, a struggle exists because the clinical intent of some products, such as prevention or treatment, might drive the product toward one benefit type over another. At the current time, his plan categorizes digital therapeutics as “experimental or investigational, and, per our benefit design, the financial liability falls to the member.” With the aforementioned physical therapy app, Evans reported that his plan coverage was under the medical benefit, but this was not without cost barriers for patients. “Medicare members had a 20% coinsurance, up to the maximum $3000 per year. We charged them 20% of the cost on the medical benefit, [and] that was a little bit of a barrier because that’s a one-time upfront cost of 20%.” In comparison, a different set of considerations arises when it comes to benefit design and coverage decisions across Medicare and commercial plans. Cannon reported that payers will wait until the CMS makes a coverage decision. Despite having no CMS guidance, Jiwanmall reported that for Medicare Advantage members, his company usually applies their commercial position and adds medical necessity or other criteria. Until such time that the CMS weighs in and provides substantial guidance on the digital therapeutic category, “you take a step back and hesitate about doing anything,” lamented Cannon. “That’s, unfortunately, [the current status] in most of the regulated markets.”
Potential Support of Digital Therapeutics by Professional Societies
Support for digital therapeutics also could be provided by professional societies, such as the American Heart Association. These societies could conduct evaluations and make recommendations. According to Evans, the providers who are members of these societies may not support the adoption of digital therapeutics because of the perception that such products could reduce practice revenue. However, Desai shared a positive outlook regarding professional society support for the nascent digital therapeutics category. “There is a lot of opportunity for engaging with the clinical community, professional societies, specialists, and primary care providers to say [that] we are here to partner with you to drive better care for patients who we mutually serve,” he said. Trust can be built, and synergy can be achieved, Desai added. Jiwanmall shared a similarly optimistic outlook in reaching out to professional societies for guidance and garnering their support for the value that these products could offer patients. Although evidential conversations might not be had given the number of new digital therapeutics in the product pipeline for the year ahead, a potential solution Jiwanmall proposed was an “overarching professional guideline” in terms of how professional societies see these products providing added clinical value; then, payers could make informed coverage decisions.
Incentivization to Drive Adoption of Digital Therapeutics
The Digital Therapeutics Alliance has been working to obtain Current Procedural Terminology (CPT) codes for remote monitoring services, Hauflaire shared, so that providers are incentivized to adopt digital therapeutics into their practices for appropriate patients. Participants cautioned that CPT codes and their structure may alienate health plans more than they incentivize a provider. Cannon and Evans noted that payers could start blocking CPT codes to take away the incentive for providers to choose digital therapeutics. In Jiwanmall’s opinion, a balance needs to be considered: on one hand, providers need to be incentivized to adopt these products, whereas on the other hand, health plans need to be incentivized to put measures and mechanisms in place to facilitate adoption from the providers. Incentivization targets may vary, from the initial prescriber who might need motivation to adopt and prescribe the product that may or may not be covered, to downstream specialists who may be managing the chronic illness over the long term. Jiwanmall called attention to the downstream impact, as these products generate data that may be leveraged beyond the initial prescriber in future management and treatment decisions. “Other specialties may come into play because of the [accumulated] data,” he explained, and these specialties could serve as a target to demonstrate improvement in clinical outcomes and for incentivization.
Another nuance that Evans pointed out is whether a provider is capitated or receives a fee for service with a particular health plan. Unlike East Coast providers, most West Coast providers are capitated and receptive to solutions that could potentially reduce their workload, Evans attested. Desai weighed in, stating that some health systems are more involved in having alternative payment models, taking on more risk, and thinking differently about care delivery; however, some remain committed to traditional fee-for-service models. “Everyone is always a little bit in both, but some are more progressive [than others],” Desai declared.
Health Policy Legislation
The COVID-19 pandemic and public health emergency accelerated the pace of innovation to address pressing challenges in health care, and new tools have subsequently been deployed and adopted, particularly in digital therapeutics. Digital therapeutics are increasingly being used to close care gaps created by provider shortages and geographic barriers in accessing physical health care systems. Participants also discussed the evolving health policy landscape and relevant legislation that has been introduced, such as the Access to Prescription Digital Therapeutics Act of 2022, which seeks to provide a framework for Medicare and Medicaid coverage of prescription digital therapeutics. This legislation would define the term “prescription digital therapeutic,” amend Section 1861(s)(2) of the Social Security Act [42 U.S.C. 1395x(s)(2)] to add “prescription digital therapeutics” to the definition of “medical and other health services” for the purposes of Medicare coverage, and set forth the Medicare coverage requirements for prescription digital therapeutics.7
The implications of such legislation for payers and other stakeholders may depend upon whether it leads to a national coverage determination stating that prescription digital therapeutics must be covered, which Evans believed may not be received favorably by payers. Alternatively, if this legislation creates a category in which payers can decide to cover prescription digital therapeutics with a specific code within the Healthcare Common Procedure Coding System, “we can decide if we want to [cover it] or not,” opined Evans. Payers nationwide are increasingly becoming more sensitive to cost and cost pressures, especially due to new legislation (eg, the Inflation Reduction Act). These factors, coupled with the possible reduction or elimination of funding for COVID-19 testing, vaccination, and treatment, could mean an “18% to 20% increase in our pharmaceutical expense for Medicare just based on the shifting of the benefit,” stated Cannon. Payers are being pushed to make health care and treatment more affordable; however, more costs are being added, including those emanating from changes in how benefits are designed. This, in turn, may force payers to eliminate any products that they are not mandated to cover. Jiwanmall predicted that CMS may place prescription digital therapeutics into a “coverage with evidence development” category, which would lead to reimbursement because “it will be the responsibility of Medicare or of the health plan that has Medicare Advantage members.” He added that this type of coverage category will allow a product to be evaluated within a Medicare-approved clinical investigation study, which could help generate much-needed evidence.
Analyzing the Digital Therapeutic Data
The participants also discussed how data accumulated from digital therapeutics could be analyzed and applied. For example, providers can evaluate data from a product to track patient adherence, and payers can evaluate population-level data to determine or discontinue coverage. According to Evans, a “positive aspect about digital [therapeutics] is [that] you can stop paying for it if people are not using it.” Cannon underscored the importance of manufacturers allowing access to data, because “the [fewer] data that [are] put in our hands, the more skeptical we become.” In today’s digital age, the assumption is that a major benefit of digital therapeutics is all the data they can provide; however, data need to be in a format that payers and other stakeholders can analyze and use. In addition to ensuring that digital therapeutics deliver clinical efficacy and safety evidence that providers and payers need, manufacturers also should consider ways to engage with health systems, Desai proposed. These forms of engagement could include piloting studies of digital therapeutic products, operationalizing the data, and demonstrating commitment that transcends the product itself and encompasses patients’ health and health care in general. Jiwanmall agreed with Desai, and he emphasized that real-world data become very appealing and valuable to payers once they are generated, analyzed over time, peer-reviewed, and published. Moreover, if these same data show economic impact, they are “gold,” Jiwanmall concluded.
Perfecting Patient Engagement
Evans explained that the “bells and whistles,” or product features, are of paramount importance because these drive patient motivation and adherence to the digital therapeutic. Cannon wondered how product features could be uniformly evaluated, understood, or even measured. He elaborated further, stating that if a digital therapeutic includes a value-add or gaming technology, he would “not know what that means,” although it is assumed that those features may reinforce product adoption. Desai pointed out that certain product features, such as gamification, may be better suited to certain patient subpopulations rather than all patients. Ultimately, the onus is on product manufacturers to research, develop, test, and perfect what works best for the target patient population.
Conclusions
Digital therapeutics are here to stay, participants agreed, although there are concerns and uncertainties, some of which are related to product adoption, usability, and health outcomes. The discussants agreed that adoption of digital therapeutics will increase, although continued conversations with all stakeholders and the development of a framework for decision-making regarding coverage will be critical, ongoing components. Participants anticipated that the adoption of digital therapeutics will disrupt and change health care; however, a divide is growing among those who welcome technological advances and those who do not. With time, the use of digital therapeutics will become easier, but, as of now, the panel agreed, the technology is far ahead of the regulatory and clinical infrastructure. •
References
1. Digital therapeutics definition and core principles. Digital Therapeutics Alliance. November 2019. Accessed October 17, 2022. https://dtxalliance.org/wp-content/uploads/2021/01/DTA_DTx-Definition-and-Core-Principles.pdf
2. Meyer-Christian J, Vanoli G, Bernhardt T, Verri C, Musci V; Deloitte; GAIA. Digital therapeutics: catalysing the future of health. Deloitte. 2021. Accessed October 17, 2022. https://www2.deloitte.com/content/dam/Deloitte/ch/Documents/life-sciences-health-care/deloitte-ch-en-lshc-digital-therapeutics.pdf
3. Ensuring appropriate quality, access, and utilization of digital therapeutics. Digital Therapeutics Alliance. April 2020. Accessed October 17, 2022. https://dtxalliance.org/wp-content/uploads/2021/01/DTx_Quality_Access_Utilization_Worksheet.pdf
4. DTx product categories. Digital Therapeutics Alliance. January 2021. Accessed October 17, 2022. https://dtxalliance.org/wp-content/uploads/2021/01/DTA_FS_DTx-Product-Categories_010521.pdf
5. Understanding DTx: a new category of medicine. Digital Therapeutics Alliance. 2022. Accessed October 17, 2022. https://dtxalliance.org/understanding-dtx/
6. Medical policy – 13.01.500 prescription digital therapeutics. Premera Blue Cross. Updated September 12, 2022. Accessed October 19, 2022. https://www.premera.com/medicalpolicies/13.01.500.pdf
7. S.3791 – Access to Prescription Digital Therapeutics Act of 2022. Congress.gov. 2022. Accessed October 17, 2022. https://www.congress.gov/bill/117th-congress/senate-bill/3791

