
- Center on Health Equity & Access
- Clinical
- Health Care Cost
- Health Care Delivery
- Insurance
- Policy
- Technology
- Value-Based Care
AJMC® Roundtable: Defining Value for the Treatment of Brain Metastases in HER2+ Metastatic Breast Cancer
This supplement was developed in conjunction with and sponsored by Seagen Inc. The supplement is based upon a roundtable meeting with A. Gajra, W. J. Gradishar, K. Kalinsky, M. Lopes, R. L. Mahtani, S. Soefje, N. Vasan, and R. D. Rao, who received a fee from Seagen Inc. The American Journal of Managed Care® also received a fee from Seagen Inc for providing editorial support.
This article was sponsored by Seagen Inc.
OVERVIEW AND BURDEN OF METASTATIC BREAST CANCER AND BRAIN METASTASES
Over 280,000 women in the United States, or 15% of the adult female population, receive a diagnosis of breast cancer each year. About 6% of these women will present with metastatic disease at the time of diagnosis. According to Ajeet Gajra, MD, MBBS, FACP, “despite advances in treatment,” the 5-year relative survival rate for metastatic breast cancer (mBC) is still less than 30%.1
Gajra stated that “there’s a greater propensity for metastatic disease in those with human epidermal growth factor receptor 2–positive [HER2+] cancer.” Approximately “15% to 20% of all patients with breast cancer have HER2+ breast cancer, which “tend[s] to [be] more aggressive [and] more likely to recur than HER2-negative [disease].2-4 Of those with mBC, a quarter are HER2+ at…diagnosis,” said Gajra.4
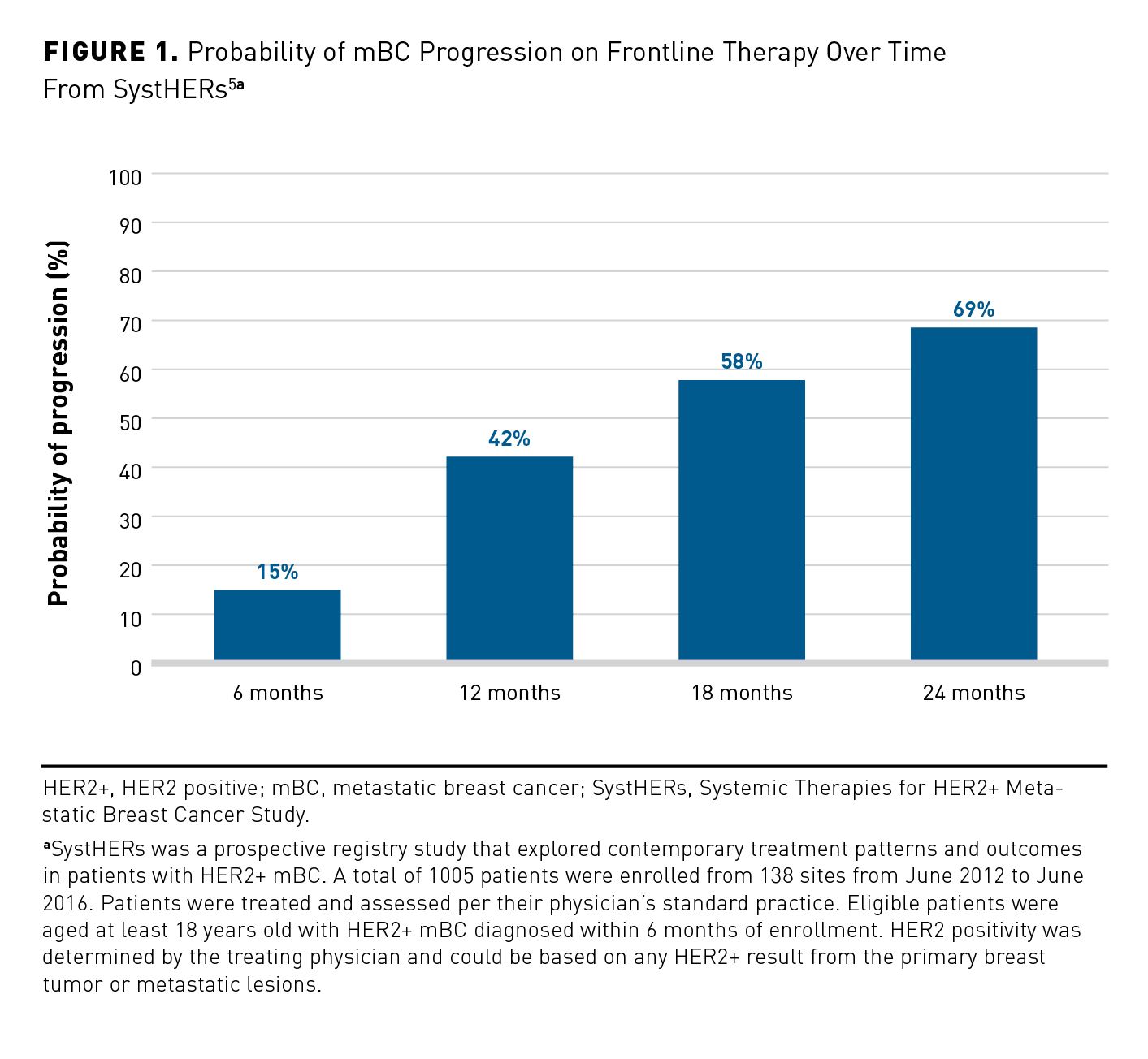
The longer patients with mBC remain on frontline therapy, the greater the likelihood of disease progression. In a retrospective analysis of claims data from the Systemic Therapies for HER2+ Metastatic Breast Cancer Study (SystHERs), patients were more than twice as likely to progress at 12 months versus 6 months and approximately 4 times as likely to progress at 24 months versus 6 months (Figure 1).5


In a study of 5709 patients with mBC, approximately 57% progressed within 12 months of receiving first-line therapy. Among those who progressed, approximately 63% started second-line treatment, 23% underwent hospice care, and approximately 13% died.6 Gajra expressed that “once there is progression in mBC, outcomes can deteriorate rapidly. [Moreover,] this demonstrates that, contrary to popular belief, many patients with mBC may…not receive second-line type therapy, which seems unimaginable in this time and age.”
Brain Metastasis
Common sites of metastasis in breast cancer include the bone, lung, liver, and brain, and “the incidence of CNS [central nervous system] metastases [in breast cancer]…has increased over time,” said Gajra.7 “Over 70% of women with advanced breast cancer…will eventually develop metastases to the bone,” he stated.8 “CNS metastases are associated with an increased risk of death…compared with other sites of metastases....9 Since 1978, the incidence of CNS metastases has more than doubled, and the incidence of liver metastases has increased as well,” Gajra said.10 According to Reshma L. Mahtani, DO, “data…suggest that upwards of almost 50% of patients, according to some series, will develop brain metastases at some time point.”11,12 An analysis of a large database for patients with HER2+ mBC determined that the average initial brain metastasis diagnosis occurred around 13 months.13 Gajra explained that “patients with HER2+ mBC are at an increased risk for brain metastases.14-16 Almost a quarter of patients have brain metastasis…at the time of diagnosis.17 Brain metastases in mBC are often characterized by early and rapid progression, thereby explaining the poor survival outcomes.”17,18 Ruta D. Rao, MD, echoed this sentiment and stated that “brain metastasis [is] a big problem in…triple-negative and…HER2+ breast cancers. Sometimes, it’s even in the patients you’ve given adjuvant treatment to, [where] their first site of relapse…is in the brain, or their only site of relapse or distant disease can be in the brain.” Mahtani added that “the incidence of CNS metastasis has doubled while our patients are living longer, their disease systemically is better controlled, and they’re living long enough to develop CNS metastasis, which we know will happen in a good proportion of patients with HER2+ and triple-negative disease.”
Results from a single-center retrospective analysis of 123 patients with HER2+ breast cancer showed that overall survival (OS) from initial breast cancer diagnosis has improved over the past few decades. “Women are living longer with…HER2+ mBC, but once brain metastases develop,…the outcomes are poor,” said Gajra.19
ECONOMIC BURDEN
Patients with HER2+ breast cancer who develop metastases experience higher costs than those with early nonmetastatic disease. In a retrospective analysis of data from the IBM MarketScan commercial database and Medicare supplemental database from 2011 to 2017, average monthly total health care costs in patients with newly diagnosed breast cancer increased sharply at the time of metastatic disease development compared with those who maintained early-stage disease. At 3 years following the diagnosis of HER2+ metastatic disease, the major cost drivers were outpatient visits and HER2-directed therapies.20
Similarly, patients with mBC who progress incur annual health care costs that are 1.6 times higher than those who do not experience progression. Patients with mBC and disease progression have nearly $50,000 more (39%) in unadjusted health care costs compared with those with who have not progressed in the past year. Moreover, earlier progression of mBC correlates with higher cumulative costs; those who experienced progression within 36 months had almost $75,000 more in health care costs than those who did not progress.6 The total cost difference was largely due to increased hospital outpatient costs and office visits.5 William J. Gradishar, MD, FASCO, FACP, acknowledged that “with respect to progression,…it’s inevitable. It doesn’t matter what kind of metastatic disease you have, you’re going to have…progression.…You never get rid of HER2-directed therapy.…We may think about abandoning other therapies, but we always try to leverage the HER2 angle, even as patients go further and further down the line of therapies, so that contributes to expense.”
The development of CNS metastases adds to the financial burden of mBC. In a retrospective cohort study of approximately 1500 patients with mBC who received HER2-targeted therapy, 1-year costs were more than twice as high among patients with brain metastasis versus those without, which were primarily driven by outpatient costs.5 Kevin Kalinsky, MD, MS, noted that “caring for the patient [for] something that is incredibly difficult to treat [has great expense].”
Interestingly, patients have reported the cost of therapy as the least important attribute of treatment. They have been far more concerned about the effectiveness of therapy and adverse effects, which can contribute to nonadherence.21
TREATMENT ADHERENCE AND HEALTH-RELATED QUALITY OF LIFE
Poor treatment adherence to first-line hormone therapy in patients with mBC is associated with a 90% increased risk of death and reduced treatment duration.22 In a cross-sectional, internet-based study of 181 patients with mBC, 33% indicated difficulties with medication adherence. According to Gajra, “it’s quite common and probably still underreported.” The highest levels of nonadherence in the study were reported in patients who had ever received hormone therapy (37.9%) and those who had ever received an oral chemotherapy agent (36.8%). Among all therapeutic modalities, the most common reasons for nonadherence or discontinuation of treatment were forgetfulness (41.3%) and intolerance of adverse events (36.5%).21 Gajra added, “Their medication [regimens] can become quite complex, [especially] if [they] have to take trastuzumab-capecitabine, and…[they experience] nausea, vomiting, [and] diarrhea; [it] can get quite confusing.” He also stated that “adherence…is not something you can completely control, and it becomes critical as more and more oral agents are becoming part of the treatment paradigm and regimens.”
Given the impact of adherence on outcomes, Maria Lopes, MD, MS, stated, “The highest-cost drug is the one that’s not even taken,” a point shared by other participants. She also added, “If somebody…fill[s] the script and then they’re not taking the drug, how sad to see that type of waste.”
Nonadherent behavior is associated with poor health-related quality of life (HRQOL). Among patients with mBC who have ever received oral chemotherapy and those currently taking oral chemotherapy, the number of nonadherent behaviors was significantly associated with a decrease in functional well-being, as assessed by Functional Assessment of Cancer Therapy-Breast (FACT-B), FACT-General, and FACT-B total scores (P < .05).21
HRQOL is lower in patients with mBC than in those with earlier-stage disease. An analysis of 464 patients with mBC from a prospective, longitudinal study, self-reported HRQOL, as measured by validated quantitative scales, was significantly affected by disease progression (P = .001). Disease progression was associated with deterioration in physical, emotional, and functional well-being; depression; reduced global quality of life; and anxiety.23
As expected, the presence of brain metastases in patients with HER2+ mBC is correlated with substantial decreases in quality of life. In a prospective US observational study of almost 1000 patients with HER2+ mBC from the SystHERs registry, those with CNS metastases at diagnosis had a lower median total FACT-B overall score compared with those without CNS metastases.18 Brain metastases substantially affect physical and emotional functioning and are associated with seizures, altered mental status, headaches, visual impairment, dizziness, ataxia, nausea, and vomiting. Gajra said that it will impair gait and worsen depression and anxiety.12,24,25
However, even more concerning is that brain metastases in patients with HER2+ disease are often silent (ie, asymptomatic) and frequently go undetected. Results from studies suggest that up to one-third of patients with brain metastases may not have any neurological symptoms.13,26,27 Mahtani noted that “[when] you look at…the percentage of patients…that…had asymptomatic brain metastases, [which] were found on screening magnetic resonance imaging [MRI] or entry into the HER2CLIMB study [NCT02614794], it’s kind of sobering to see how many patients…had brain metastasis.”
TREATMENT GUIDELINES AND OPTIONS
The goals of treatment for patients with HER2+ mBC include improving patient quality of life, extending OS, providing a meaningful response rate, and maintaining functional status, said Scott Soefje, PharmD, MBA, BCOP, FCCP, FHOPA. Mahtani said, “In the setting where you have an agent that has an OS benefit, for me, that weighs very heavily. In the situation where a patient is very symptomatic and you need a response quickly, overall response rate is important.”
The American Society of Clinical Oncology has recommendations for the treatment of patients with HER2+ mBC in the first- and second-line settings based on results from large, randomized controlled trials.
The phase 3, randomized, placebo-controlled CLEOPATRA trial (NCT00567190) in over 800 patients with HER2+ mBC demonstrated an OS benefit with first-line pertuzumab in combination with trastuzumab and docetaxel compared with placebo, trastuzumab, and docetaxel (median OS, 56.5 vs 40.8 months, respectively).28 EMILIA, a phase 3, randomized, open-label trial in patients with HER2+ unresectable, locally advanced, or mBC previously treated with trastuzumab and a taxane evaluated trastuzumab emtansine (T-DM1) versus lapatinib and capecitabine (ie, control) in the second-line setting (NCT00829166). T-DM1 was associated with a median OS benefit of 29.9 months compared with 25.9 months in the control group.29
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®)
The National Comprehensive Cancer Network® (NCCN®) offers recommendations for preferred lines of therapy in recurrent stage IV HER2+ breast cancer. The NCCN Guidelines® for the third line and beyond include several options. The combination of tucatinib, trastuzumab, and capecitabine is a category 1 recommendation and is preferred in patients with both systemic and CNS progression on T-DM1.a Gajra indicated that the tucatinib regimen was a category 1 recommendation. “Technically, if you go by the label, [tucatinib] is…second-line [therapy],” Gajra said. He also remarked that “notably, every [other recommended regimen] is a category 2.” It is important to note that the NCCN Guidelines for Breast Cancer recommend brain MRI if the patient displays symptoms suspicious for CNS metastasis.30
NCCN Guidelines for CNS
NCCN Guidelines for CNS in HER2+ mBC include the category 1 recommendation of tucatinib plus trastuzumab plus capecitabine if the patient previously received 1 or more anti-HER2-based regimens. Lapatinib-capecitabine, neratinib-capecitabine, and ado-trastuzumab emtansine are category 2A options for HER2+ mBC. Gajra stated that “per NCCN, ongoing CNS surveillance with brain MRIs is essential to allow early interventions in the case of progression or inadequate response.”31
Rao pointed out that “until recently, there was…very limited information [in] the CNS guidelines for breast cancer.” Like others, she indicated “that [her] preferred regimen…[for brain metastases] would be tucatinib-trastuzumab-capecitabine, [and so] I don’t necessarily go to the NCCN Guidelines for CNS to confirm that. But it’s always good to see what’s in them.” When asked whether there is room for the NCCN Guidelines for Breast Cancer to more closely match the CNS guidelines in the future, Gradishar stated that “neuro-oncologists and breast oncologists don’t occupy the same space, oftentimes physically or in [thought].” He felt it would be best for them “to complement each other without going too far afield so that there [is] discordance between the 2.” Gradishar hopes that over time they will have more data that may justify having complete synchronization between the 2 pathways.
Sequencing Treatment and Management of Brain Metastasis
Neil Vasan, MD, PhD, and others concurred that the CLEOPATRA and EMILIA regimens are frequently used in the first- and second-line settings, respectively. However, Gradishar noted that “as we go forward, obviously a lot of...drugs are vying to move up and displace T-DM1, so what we talk about today may be old news in a year…and I think the sequences, it’s not going to be solved easily.” According to Kalinsky, “this [is] an evolving field, and certainly as our systemic therapies get better, some don’t always have great CNS penetration.” Rao stated that if there “is progression in the body and the brain, and [we] have exhausted local therapies for the brain metastasis…that’s a situation where it’s easy to come to the decision that we need to switch their systemic therapy and try to find something that would target the brain metastasis as well.” Mahtani noted that some patients can have very long periods of disease control with first- or second-line therapy; however, “other patients have a more aggressive clinical course with…brain metastasis much earlier…and…[are] more resistant to therapy. I think it becomes quickly apparent which bucket [the patient] falls in.”
Vasan stated that “around the third line is when I start to think more about where the disease is, if it’s the CNS versus the body.… In the second-line setting, if someone develop[s] CNS disease, the FDA-approved indication for tucatinib is after 1 or more lines of anti-HER2 therapy in the metastatic setting. I have treated patients in the second-line setting with extensive CNS disease, or maybe CNS disease where they couldn’t get a complete resection.”
Vasan and Kalinsky communicated that tucatinib or trastuzumab deruxtecan is often considered in the third-line setting. Mahtani added that she would even consider using tucatinib in the third-line setting in patients without brain metastases, especially “if I am not feeling that there are [adherence] issues and they’d be fine with an oral regimen and they prefer an oral regimen.”
“I think of margetuximab as more fourth line right now, although…it just became approved…and we don’t have a lot of experience with this drug outside clinical trials,” said Vasan. Kalinsky agreed with his sentiment. Mahtani acknowledged that “most…patients, not all, but many of them will end up seeing all these therapies in some sort of sequence, and it’s just trying to optimize that sequence that may be unique for each individual patient based on their preference for oral versus intravenous, their ability to [adhere to] a treatment, their disease burden, and their sites of disease.”
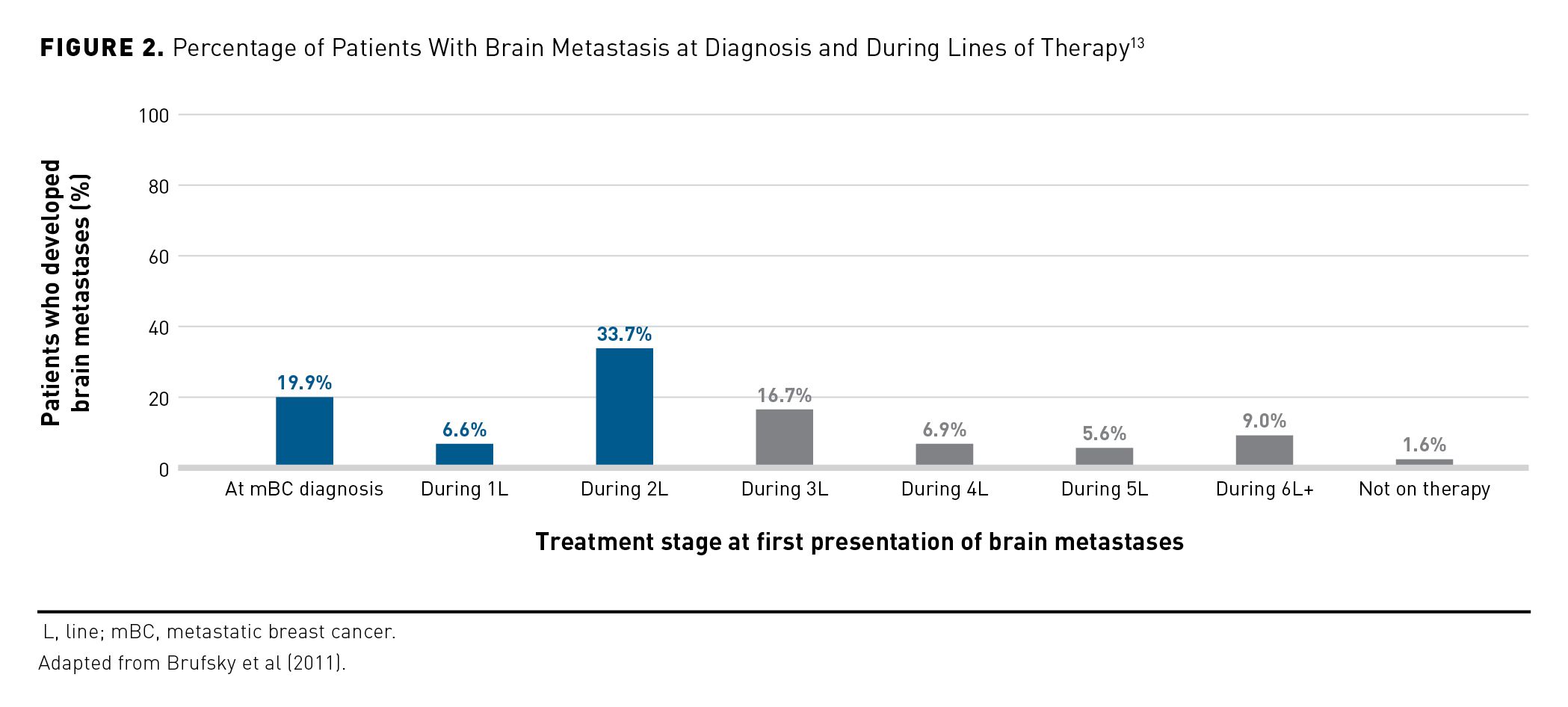
Although many clinicians start considering using CNS-active agents in the third line, evidence suggests that earlier use is warranted. In a retrospective review of medical records, patients had a high risk (42%) of developing CNS metastasis while receiving trastuzumab as a first-line therapy; trastuzumab does not cross the blood-brain barrier. Additionally, more than 33% of women developed symptomatic CNS metastases while receiving trastuzumab-based therapy, often while their other systemic disease was responding or stable. Because these patients were receiving first-line therapy, the authors concluded that the high incidence of CNS metastasis was not related to the number of prior lines of treatment.32 According to Gajra, the “development of brain metastases should be considered throughout the stages of mBC.” Over 60% of patients with HER2+ mBC who develop brain metastases may do so as early as the second line of therapy (Figure 2).13


Role of Tyrosine Kinase Inhibitors in the Treatment Paradigm
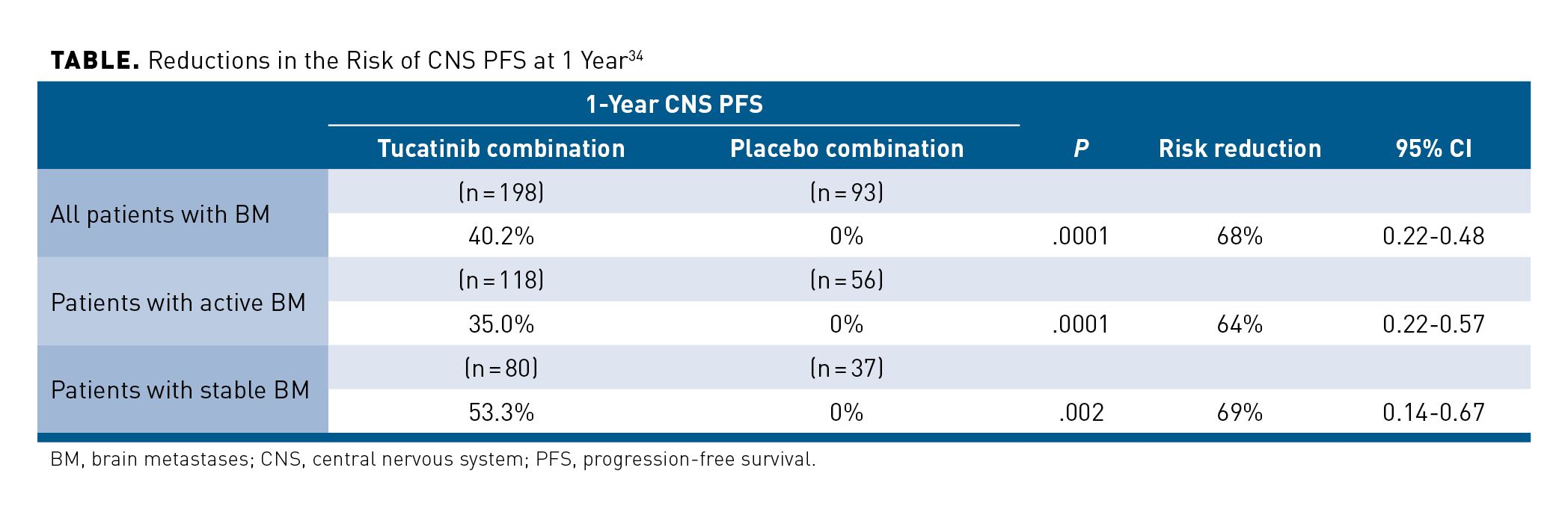
Although patients with HER2+ mBC are at increased risk for brain metastases, further evidence is needed to support a change in the treatment paradigm to broader, earlier use of tyrosine kinase inhibitors (TKIs) (eg, tucatinib) and other agents with CNS penetration. Several TKIs are included in the NCCN treatment recommendations for HER2+ mBC with brain metastasis.30 However, Kalinsky and others indicated that tucatinib has emerged as the preferred TKI. He acknowledged that “questions [still]remain…in terms of whether there are other partners that can be given with tucatinib.” Mahtani stated that she no longer utilizes neratinib in the metastatic setting since the availability of tucatinib. “I think in terms of tolerability, tucatinib is much better tolerated,” she said. Vasan indicated that “some issues that I’ve come into…are diarrhea and whether to dose-reduce tucatinib versus capecitabine. I think that’s a common scenario…[but]…it’s small numbers.” However, he noted that diarrhea with neratinib or lapatinib in combination with capecitabine is more difficult to control. As previously discussed, several clinicians mentioned that tucatinib may be incorrectly labeled by some as a drug to be used in HER2+ mBC with brain metastases only. “[HER2CLIMB was] a phase 3 trial that showed efficacy broadly, not just in patients with brain metastases,” said Gradishar. One-year progression-free survival (PFS) was significantly higher in the tucatinib combination group (33.1%) compared with the placebo combination group (12.3%; P < .001).33 Approximately 50% of the trial population had brain metastasis, with a large proportion of those patients having untreated brain metastases. The tucatinib combination was associated with a significant reduction (68%) in the risk of CNS progression or death compared with the placebo combination (HR, 0.32; 95% CI, 0.22-0.48; P < .0001) (Table).34 The study authors acknowledged that HER2CLIMB was the first double-blind, randomized trial of systemic therapy to show clinically meaningful gains in OS in patients with brain metastases, including those with active brain metastases.34


Several participants agreed that earlier use of tucatinib (ie, in the second line) would be considered (eg, for patients with extensive progression in the brain). “I’ve seen activity that is pretty remarkable in terms of shrinkage of brain metastases and very much on par with what we saw in the HER2CLIMB study,” Mahtani stated. However, clinicians are reluctant to use tucatinib prior to T-DM1. According to Mahtani, “100% of the patients [in] HER2CLIMB had seen T-DM1 in some setting. And there comes this issue of sequencing and [not] knowing what activity you’re going to get with T-DM1 if you use tucatinib in advance.…In a patient that has rapid progression in the brain, and that seems to be the site that really is going to dictate their overall prognosis…you can make a case there for using tucatinib.”
SCREENING GUIDELINES AND CONSIDERATIONS FOR PATIENTS WITH BRAIN METASTASIS
As Mahtani stated, current “guidelines don’t call for routine brain MRIs and screening” in all patients with HER2+ mBC. NCCN Guidelines and other studies recommend brain MRI in patients who are experiencing symptoms suggestive of CNS metastasis.25,30 As such, some clinicians noted that they do not look for brain metastasis unless they have suspicion.
However, Gradishar suggested that “there’s probably going to be a significant uptick in the use of MRIs.” He acknowledged that “based on…newer data, there is…discussion [among members of the NCCN] that’s ongoing about whether we should mandate or recommend or consider strongly…[brain imaging] to give [physicians] some wiggle room to order tests if [they] want to get [them]. [But,] I don’t think we’re there yet.” Further, Gradishar said that it needs to be “demonstrate[d] that, by finding these things early, we can translate that into actionable things that result in a better outcome.” These outcomes include quality-of-life measures, as current debate centers on whether patients want to know about progression to the brain, especially if they are asymptomatic or have very small lesions. According to Rao, “the question is…with the lead time…with the patient knowing about them earlier, the physician knowing about them earlier, and earlier treatment: Is that going to improve their quality of life, and…OS?” Mahtani believes that patient-reported outcomes data are important. Although she acknowledged the anxiety surrounding a brain metastasis diagnosis in patients who are not experiencing symptoms, “the flip side of that is saving [a patient] the experience of going through…progression…having a seizure in front of a child, having some sort of neurological episode that could be…very traumatic for the patient and…family.”
When asked whether all patients with breast cancer should be treated as if they are at risk of brain metastases, Mahtani stated “that all patients with HER2-positive [breast cancer] are at risk for brain metastasis, so the best treatment is prevention.…If we could get an agent like tucatinib or utilize neratinib more selectively in high-risk patients, we could possibly prevent brain metastasis, and I would be in favor of that strategy.…I think we should have a low threshold to scan these patients and recognize that this is an area [where] they often have metastatic disease manifest.” Gradishar agreed with Mahtani “about treating brain metastasis…like preventive health care in general. If we can prevent brain metastasis, that would be a great thing, and we’ll have to see if we get hints of that from some of the early-stage trials.”
Vasan indicated that although he would not treat all patients with mBC as if they are at risk of brain metastasis, he would consider it in a patient who experienced progression. He explained that screening patients for brain metastases in the first-line setting is not known to be effective; however, “if there were high-quality data that supported [screening with later line settings], people may shift their practice.”
One of the obstacles to improved screening is payer coverage. As Mahtani noted, “if someone’s progressing systemically, I want to know what’s going on in their brain. And if I could get it covered, I would try to get it done.” As a payer, Lopes recognizes the “unmet need around better surveillance, better identification, and detection” and would hope that “the clinical utility of what you’re finding…ties to treatment options that circle back to improving survival, reduc[ing]…costs,…[and] adding value…in terms of response…and quality of life.”
When asked what data are needed to guide treatment selection for brain metastases, Gradishar said, “The issue is going to be if you can tease out a CNS OS or PFS that’s meaningful.…Many patients will [receive]…other therapies or their brain disease may stay stable for some period…[but] that doesn’t necessarily mean that their other disease will [remain stable]. [It will be] challenging to…figure out whether…other drugs are going to have a CNS effect [and I doubt] there are going to be numerous phase 3 trials that are similar in design to…HER2CLIMB [that] address [it] very rigorously.”
ROLE OF GUIDELINES IN DRUG COVERAGE
Guidelines are critical to payers when developing drug policies. Lopes stated that “oncology is a protected class.…As…we’re looking at the different treatment modalities, we’re looking to be evidence based.…We…are looking at not only the FDA label but [also] appropriate off-label use. [The] NCCN [Guidelines are] usually the most comprehensive and updated source that we’ll reference in defense of approval or denial.…To the extent [that] those guidelines are updated regularly…the more conformity, the more consensus around [them]…may also give physicians [the] opportunity to manage care.” She also pointed out that many payers outsource radiology to third-party vendors who use guidelines to define prior authorization criteria. Clear guidelines make it easier for payers to accept these costs.
Conversely, clinicians use guidelines more as a guardrail along with their clinical experience. “The guidelines are in particular something that’s utilized by payers.…[They are] something that is really incorporated in that decision-making,” said Kalinsky. According to Rao, “the guidelines are exactly [that]…they’re guidelines. When you want to give a certain treatment and…it falls within the guidelines…it is much easier to get the regimen approved…It also put[s]…clinical trial data into…context.” Soefje added that his “pharmacists are…trained…to question if something comes through and it is not guideline supported.” It doesn’t imply that they will stop a request, but they will make sure that something was not entered by mistake, he said.
It was also noted that payers and providers need comparative efficacy data between agents to further support decision-making and drug coverage.
IMPROVING PATIENT MANAGEMENT
Several clinicians pointed out that integrated care is key in managing patients with mBC and CNS metastases. Kalinsky stated that “a multidisciplinary approach, where we have incorporation of [a] neurologist, neurosurgeons, [and] radiation oncologist” is beneficial, depending on the case. Lopes recommended “a team-based approach that includes a clinical pharmacist [and] a care manager…because a lot of these patients…[are] high risk [and]…high cost.…The integration of services…become[s] critically important to identify patient needs [and] even social determinants of health. This team approach…also supports the Oncology Care Model, and the patient-centered medical home or advanced medical home.” She also noted that it can identify barriers to nonadherence and individualize care, as many of these patients have comorbidities or financial issues.
Support Services for Patients
Lopes described some digital solutions that may support patient-centered care. Some of these apps track information on issues such as nausea, vomiting, pain, behavioral health issues, sleep, anxiety, and depression. “Can this [information] integrate seamlessly into the care delivery model and can we have better and more real-time shared decision-support tools for…improving quality of life and maybe even reducing unnecessary and avoidable emergency department visits or hospitalizations?” she questioned.
Adherence
Vasan suggested the need for better ways to manage the burdens of tolerability and adherence associated with some of the therapies. Rao indicated “the importance of having…family members there to help with adherence and even management of [adverse] effects. For the patients who could use…extra support [ie, those with severe cognitive impairment], we really haven’t been able to have [a family member] come into clinic with them [because of COVID-19 protocols].…We’re on the west side of Chicago, so a lot of these tools and information would be nice, but a lot of our patients don’t have access to [the] internet or online tools to adhere to drug regimens.”
Soefje described that, in his area, pharmacist-run clinics have been set up “that are monitoring oral chemotherapy. We almost see them very similarly to the Coumadin-type clinics where patients started on the therapy. The pharmacist has a defined protocol to follow and then we follow those patients sometimes even for an extended period of time. We started it with the CDK4/6 inhibitors but we’re beginning to expand it into other areas. When we combine the pharmacist and the clinic with our specialty pharmacy group, we have cost savings and touch points with patients over the course of their therapy.” He also discussed how they are developing technology, such as text messaging and smart phone applications, to help with adherence issues (eg, treatment adverse effects and their management). The system will incorporate pharmacists, providers, and nurses. Soefje believes that such programs are “the future of adherence modification.”
Similarly, Rao indicated that they “have oral pharmacists who specialize in the oral therapy dedicated to certain disease sites” [such as the] “breast, and [they are] very helpful in…educating…patients when they first start [a] regimen. This is true for the HER2CLIMB regimen [and] patients on CDK4/6 inhibitors in the HER+ metastatic setting.…Patients often reach out to [them] or…our clinic nurses [about] any [adverse] effects.”
CONCLUSIONS
The development of brain metastases in mBC is associated with poor survival outcomes, reduced quality of life, and increased costs. Although many patients with HER2+ mBC and brain metastases experience neurologic symptoms, up to one-third of patients are asymptomatic and their brain metastases remain undetected. Moreover, approximately 60% of patients with HER2+ mBC who develop brain metastases may do so as early as the second line of therapy. Despite these findings, more evidence is needed to support a change in the treatment paradigm to broader, earlier use of TKIs (eg, tucatinib) and other agents with CNS penetration. Although current guidelines do not recommend brain MRIs and screening for those without CNS symptoms, several clinicians noted that all patients with HER2+ mBC are at risk for brain metastasis and that the best treatment would be prevention. Comparative efficacy data between agents is needed to further support decision-making and drug coverage. Multidisciplinary, integrated care is essential to managing patients with mBC and brain metastases. Patient support services, including those for treatment adherence and the management of adverse events, are also key to improving outcomes in mBC with brain metastases.
aThe tucatinib, trastuzumab, and capecitabine regimen can also be used per NCCN guidelines in second-line therapy.
REFERENCES
1. Cancer stat facts: female breast cancer. National Cancer Institute. Accessed April 29, 2021. https://seer.cancer.gov/statfacts/html/breast.html
2. Cancer stat facts: female breast cancer subtypes. National Cancer Institute. Accessed April 29, 2021. https://seer.cancer.gov/statfacts/html/breast-subtypes.html
3. Musolino A, Ciccolallo L, Panebianco M, et al. Multifactorial central nervous system recurrence susceptibility in patients with HER2-positive breast cancer: epidemiological and clinical data from a population-based cancer registry study. Cancer. 2011;117(9):1837-1846. doi:10.1002/cncr.25771
4. Gong Y, Liu YR, Ji P, Hu X, Shao ZM. Impact of molecular subtypes on metastatic breast cancer patients: a SEER population-based study. Sci Rep. 2017;7:45411. doi:10.1038/srep45411
5. Seagen. Data on file. 2020.
6. Reyes C, Engel-Nitz NM, DaCosta Byfield S, et al. Cost of disease progression in patients with metastatic breast, lung, and colorectal cancer. Oncologist. 2019;24(9):1209-1218. doi:10.1634/theoncologist.2018-0018
7. Kennecke H, Yerushalmi R, Woods R, et al. Metastatic behavior of breast cancer subtypes. J Clin Oncol. 2010;28(20):3271-3277. doi:10.1200/JCO.2009.25.9820
8. Manders K, van de Poll-Franse LV, Creemers GJ, et al. Clinical management of women with metastatic breast cancer: a descriptive study according to age group. BMC Cancer. 2006;6:179. doi:10.1186/1471-2407-6-179
9. Agostinetto E, Masci G, Giordano L, et al. HER2-positive breast cancer and CNS metastases: prognostic factors and clinical outcome. Ann Oncol. 2019;30(suppl 3):iii60. doi:10.1093/annonc/mdz100.037
10. van den Hurk CJ, Eckel R, van de Poll-Franse LV, et al. Unfavourable pattern of metastases in M0 breast cancer patients during 1978-2008: a population-based analysis of the Munich Cancer Registry. Breast Cancer Res Treat. 2011;128(3):795-805. doi:10.1007/s10549-011-1372-y
11. Leyland-Jones B. Human epidermal growth factor receptor 2-positive breast cancer and central nervous system metastases. J Clin Oncol. 2009;27(31):5278-5286. doi:10.1200/JCO.2008.19.8481
12. Bachelot T, Romieu G, Campone M, et al. Lapatinib plus capecitabine in patients with previously untreated brain metastases from HER2-positive metastatic breast cancer (LANDSCAPE): a single-group phase 2 study. Lancet Oncol. 2013;14(1):64-71. doi:10.1016/S1470-2045(12)70432-1
13. Brufsky AM, Mayer M, Rugo HS, et al. Central nervous system metastases in patients with HER2-positive metastatic breast cancer: incidence, treatment, and survival in patients from registHER. Clin Cancer Res. 2011;17(14):4834-4843. doi:10.1158/1078-0432.CCR-10-2962
14. Azim HA, Abdel-Malek R, Kassem L. Predicting brain metastasis in breast cancer patients: stage versus biology. Clin Breast Cancer. 2018;18(2):e187-e195. doi:10.1016/j.clbc.2017.08.004
15. Genre L, Roché H, Varela L, et al. External validation of a published nomogram for prediction of brain metastasis in patients with extra-cerebral metastatic breast cancer and risk regression analysis. Eur J Cancer. 2017;72:200-209. doi:10.1016/j.ejca.2016.10.019
16. Hung MH, Liu CY, Shiau CY, et al. Effect of age and biological subtype on the risk and timing of brain metastasis in breast cancer patients. PLoS One. 2014;9(2):e89389. doi:10.1371/journal.pone.0089389
17. Vidal GA, Debusk K, Gautam G, Vlahiotis A, Fisher M, Pulgar S. Occurrence of brain metastasis and treatment patterns among patients with HER2-positive metastatic breast cancer. Presented at: ESMO Breast Cancer Virtual Meeting; May 23-24, 2020. Abstract 174P. Accessed May 13, 2021. https://oncologypro.esmo.org/meeting-resources/esmo-breast-cancer-virtual-meeting-2020/occurrence-of-brain-metastasis-and-treatment-patterns-among-patients-with-her2-positive-metastatic-breast-cancer
18. Hurvitz SA, O’Shaughnessy J, Mason G, et al. Central nervous system metastasis in patients with HER2-positive metastatic breast cancer: patient characteristics, treatment, and survival from SystHERs. Clin Cancer Res. 2019;25(8):2433-2441. doi:10.1158/1078-0432.CCR-18-2366
19. Mounsey LA, Deal AM, Keith KC, et al. Changing natural history of HER2-positive breast cancer metastatic to the brain in the era of new targeted therapies. Clin Breast Cancer. 2018;18(1):29-37. doi:10.1016/j.clbc.2017.07.017
20. Sussell JA, Sheinson D, Wu N, Shah-Manek B, Seetasith A. HER2-positive metastatic breast cancer: a retrospective cohort study of healthcare costs in the targeted-therapy age. Adv Ther. 2020;37(4):1632-1645. doi:10.1007/s12325-020-01283-4
21. daCosta DiBonaventura M, Copher R, Basurto E, Faria C, Lorenzo R. Patient preferences and treatment adherence among women diagnosed with metastatic breast cancer. Am Health Drug Benefits. 2014;7(7):386-396.
22. Barron TI, Kennedy MJ, Sharp L, Bennett K. P1-08-12: hormonal therapy compliance and mortality in metastatic breast cancer. Cancer Res. 2011;71(suppl 24):P1-08-12. doi:10.1158/0008-5472.SABCS11-P1-08-12
23. Marschner N, Zacharias S, Lordick F, et al. Association of disease progression with health-related quality of life among adults with breast, lung, pancreatic, and colorectal cancer. JAMA Netw Open. 2020;3(3):e200643. doi:10.1001/jamanetworkopen.2020.0643
24. Cacho-Díaz B, Spínola-Maroño H, Arrieta VA, et al. Diagnosis of brain metastases in breast cancer patients resulting from neurological symptoms. Clin Neurol Neurosurg. 2018;173:61-64. doi:10.1016/j.clineuro.2018.08.002
25. Oltean D, Dicu T, Eniu D. Brain metastases secondary to breast cancer: symptoms, prognosis and evolution. Tumori. 2009;95(6):697-701. doi:10.1177/030089160909500610
26. Miller KD, Weathers T, Haney LG, et al. Occult central nervous system involvement in patients with metastatic breast cancer: prevalence, predictive factors and impact on overall survival. Ann Oncol. 2003;14(7):1072-1077. doi:10.1093/annonc/mdg300
27. Niwinska A, Tacikowska M, Murawska M. The effect of early detection of occult brain metastases in HER2-positive breast cancer patients on survival and cause of death. Int J Radiat Oncol Biol Phys. 2010;77(4):1134-1139. doi:10.1016/j.ijrobp.2009.06.030
28. Swain SM, Baselga J, Kim SB, et al; CLEOPATRA Study Group. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med. 2015;372(8):724-734. doi:10.1056/NEJMoa1413513
29. Diéras V, Miles D, Verma S, et al. Trastuzumab emtansine versus capecitabine plus lapatinib in patients with previously treated HER2-positive advanced breast cancer (EMILIA): a descriptive analysis of final overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2017;18(6):732-742. doi:10.1016/S1470-2045(17)30312-1.
30. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Breast cancer V.5.2021. © National Comprehensive Cancer Network, Inc. 2020. All rights reserved. Accessed August 3, 2021. To view the most recent and complete version of the guideline, go online to NCCN.org.a
31. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Central nervous system cancers V.1.2021. © National Comprehensive Cancer Network, Inc. 2020. All rights reserved. Accessed May 13, 2021. To view the most recent and complete version of the guideline, go online to NCCN.org.a
32. Bendell JC, Domchek SM, Burstein HJ, et al. Central nervous system metastases in women who receive trastuzumab-based therapy for metastatic breast carcinoma. Cancer. 2003;97(12):2972-2977. doi:10.1002/cncr.11436
33. Murthy RK, Loi S, Okines A, et al. Tucatinib, trastuzumab, and capecitabine for HER2-positive metastatic breast cancer. N Engl J Med. 2020;382(7):597-609. doi:10.1056/NEJMoa1914609
34. Lin NU, Borges V, Anders C, et al. Intracranial efficacy and survival with tucatinib plus trastuzumab and capecitabine for previously treated HER2-positive breast cancer with brain metastases in the HER2CLIMB trial. J Clin Oncol. 2020;38(23):2610-2619. doi:10.1200/JCO.20.00775


